Harnessing behavioural science to implement the National Overprescribing Review recommendations - Sion Scott, Lecturer in Behavioural Medicine, University of Leicester & Debi Bhattacharya, Professor of Behavioural Medicine, University of Leicester
The National Overprescribing Review estimates that 10% of medicines prescribed in primary care are unnecessary or harmful(1). The review concludes that overprescribing is caused by systemic and cultural factors. Failure to embed deprescribing into the prescribing process is a significant contributor to overprescribing. The principles of Good Prescribing Practice (Figure 1) require prescribers to monitor the appropriateness of the medicines they prescribe and proactively deprescribe any that become inappropriate before they cause harm. Despite this, deprescribing in both primary and secondary care is largely ‘reactive’ in response to an adverse drug event such as a side effect(2,3). Practitioner motivation to reactively deprescribe is likely to be very high given that inaction leads to certain patient harm. For example, reactively deprescribing an anticoagulant for a patient presenting with a gastric bleed. Proactive deprescribing, however, requires a complex weighing of future potential harm versus benefit(3). Uncertainties regarding the likely benefits and potential harms is a barrier to proactive deprescribing(4). For example, a practitioner may be reticent to proactively deprescribe an antihypertensive for a patient even if the risk of falling and resulting fracture is greater than the risk of a cardiovascular event.

Figure 1 Principles of Good Prescribing Practice (5)
One strategy proposed for identifying and resolving overprescribing is the introduction of Structured Medication Reviews. These are a review of all medicines that a patient is using to assess them for safety, effectiveness and tailored to the patient’s needs. Structured Medication Reviews are intended to ‘take considerably longer than an average GP appointment’ and be primarily undertaken by prescribing pharmacists thus introducing extra resource for increasing deprescribing activity in primary care.
Stakeholder engagement is essential for achieving behaviour change, however, purely focussing on what people think they need to deliver the change, often fails to address all barriers and enablers(6). Staff commonly cite the need for extra resource as the solution. However, given extra resource such as time and workforce, staff will often increase existing activities with which they are familiar and have a known pathway of recognition rather than undertake the desired new behaviour. Another commonly delivered ‘solution’ to effect a change in practice is education and training. Whilst having the required knowledge and skills is clearly essential, behaviour change is rarely achieved by addressing only these barriers/enablers (6).
Asking staff what help they think they need, places the onus on them to correctly identify their barriers and enablers to undertaking the desired behaviour and then select the most appropriate solutions. The field of behavioural science has offered a scientific approach to garner meaningful input from stakeholders to shape the development of strategies to support implementation of a new behaviour(7). Stakeholders’ thoughts and concerns regarding the required change in practice can be analysed to identify and prioritise the key barriers/enablers to implementing a new behaviour(8). For each key barrier/enabler, a range of theory and evidence based solutions have been collated into a taxonomy(9). Stakeholders can then be facilitated to select solutions from the taxonomy according to criteria such as the extent to which it is likely to be acceptable to everyone, affordable for the organisation and not introduce inequity(10).
Applying behavioural science to address the determinants of opioid deprescribing in primary care has identified six key components needed to support prescribers(11). Figure 2 provides these six components that are yet to be included in all primary care strategies.
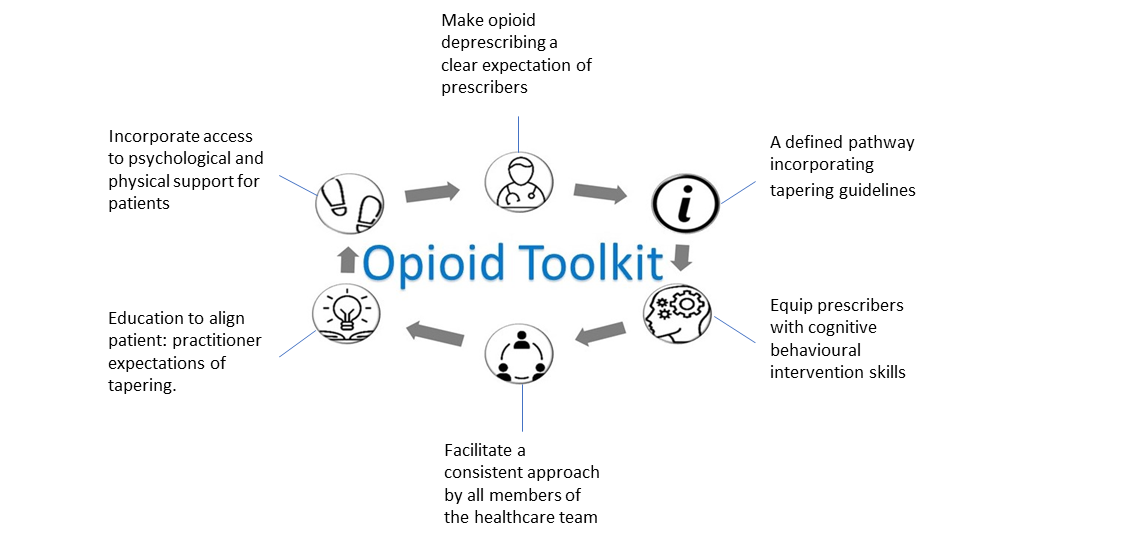
Figure 2 Opioid toolkit
Whilst there is likely to be some overlap between the determinants of opioid deprescribing and proactive deprescribing in the primary care context, they are not the same behaviour. For example, patient reluctance to have their opioids deprescribed is addressed in the toolkit through education to modify unrealistic patient expectations of pain management and opioid tapering(11). In contrast, patients expect prescribers to proactively deprescribe(12). However, stakeholder engagement with prescribers identified that a barrier to them proactively deprescribing is the belief that patients are resistant(13). Accordingly, the component to address this barrier should target the practitioners’ misconception.
The determinants of proactive deprescribing in the hospital context have been fully characterised and an intervention co-designed by a team comprising experts in behavioural science working with patients, geriatricians and pharmacists(10). The National Institute for Health Research funded CHARMER (CompreHensive geriAtRician-led MEdication Review) study will evaluate the intervention across up to 42 NHS hospitals. This will provide the evidence for the safety, effectiveness and cost-effectiveness of proactive deprescribing which is essential to underpin commissioning decisions. Differences between the primary and secondary care contexts are likely to yield different determinants and therefore the CHARMER intervention is unlikely to be suitable for implementation in primary care. The CHARMER research programme, however, provides a blueprint for primary care teams to work with experts in behavioural science to implement the National Overprescribing Review recommendations and evaluate any resulting interventions for their safety, effectiveness and cost per quality adjusted life year as there are no pre-existing trials delivering data on all three aspects.
References
- Good for you, good for us, good for everybody: A plan to reduce overprescribing to make patient care better and safer, support the NHS, and reduce carbon emissions [Internet]. Department of Health and Social Care; 2021 [cited 2021 Dec 21]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1019475/good-for-you-good-for-us-good-for-everybody.pdf
- Anderson K, Foster M, Freeman C, Luetsch K, Scott I. Negotiating “unmeasurable harm and benefit”: perspectives of general practitioners and consultant pharmacists on deprescribing in the primary care setting. Qualitative health research. 2017;27(13):1936–47.
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Deprescribing admission medication at a UK teaching hospital; a report on quantity and nature of activity. International journal of clinical pharmacy. 2018;40(5):991–6.
- Scott S, Wright DJ, Bhattacharya D. The role of behavioural science in changing deprescribing practice. Br J Clin Pharmacol. 2021 Jan;87(1):39–41.
- General Medical Council. Good practice in prescribing and managing medicines and devices [Internet]. 2021 [cited 2021 Dec 16]. Available from: https://www.gmc-uk.org/-/media/documents/prescribing-guidance-updated-english-20210405_pdf-85260533.pdf
- Kelly MP, Barker M. Why is changing health-related behaviour so difficult? Public health. 2016;136:109–16.
- Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. bmj. 2021;374.
- Scott S, Twigg MJ, Clark A, Farrow C, May H, Patel M, et al. Development of a hospital deprescribing implementation framework: a focus group study with geriatricians and pharmacists. Age and ageing. 2020;49(1):102–10.
- Johnston M, Carey RN, Connell Bohlen LE, Johnston DW, Rothman AJ, de Bruin M, et al. Development of an online tool for linking behavior change techniques and mechanisms of action based on triangulation of findings from literature synthesis and expert consensus. Translational behavioral medicine. 2021;11(5):1049–65.
- Scott S, May H, Patel M, Wright DJ, Bhattacharya D. A practitioner behaviour change intervention for deprescribing in the hospital setting. Age and ageing. 2021;50(2):581–6.
- Bhattacharya D. Reducing opioid use for chronic non-cancer pain in primary care. Prescriber. 2021;32(5):28–31.
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Attitudinal predictors of older peoples’ and caregivers’ desire to deprescribe in hospital. BMC geriatrics. 2019;19(1):1–11.
- Anderson K, Stowasser D, Freeman C, Scott I. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: a systematic review and thematic synthesis. BMJ open. 2014;4(12):e006544.
Content provided by Sion Scott Lecturer in Behavioural Medicine, University of Leicester & Debi Bhattacharya Professor of Behavioural Medicine, University of Leicester
A spotlight on Pulse Oximetry - Not all pulse oximeters are created equally! - Dr. Basil Matta MA FRCA FFICM, Senior Medical Director, Masimo
 The first commercially available pulse oximeter, a life-saving device that clipped on a finger and showed the level of oxygen in blood, was invented by Dr. Takuo Aoyagi, a Japanese Bioengineer in 1974. Monitoring of blood oxygen saturation is one of the greatest advances in patient monitoring and the introduction of this technology coincided with a 90% reduction in anesthesia-related fatalities. Over the course of the past almost 50 years, the ability to detect oxygen saturation levels has become as important if not more important that the other 4 vital signs—temperature, blood pressure, pulse rate, and respiratory rate.
The first commercially available pulse oximeter, a life-saving device that clipped on a finger and showed the level of oxygen in blood, was invented by Dr. Takuo Aoyagi, a Japanese Bioengineer in 1974. Monitoring of blood oxygen saturation is one of the greatest advances in patient monitoring and the introduction of this technology coincided with a 90% reduction in anesthesia-related fatalities. Over the course of the past almost 50 years, the ability to detect oxygen saturation levels has become as important if not more important that the other 4 vital signs—temperature, blood pressure, pulse rate, and respiratory rate.
COVID-19 has shone a spotlight on this most important measurement in medical practice, with media outlets suddenly showing interest in these devices. The demand, influenced by COVID-19, has also led to many less efficacious pulse oximeters being marketed and bought by lay people as well as poorly informed health care providers. The vast majority of these poor quality oximeters have not undergone proper testing and their performance falls far short of what is expected from hospital grade devices that are designed to prevent serious deterioration and death.
With heightened awareness of pulse oximetry technology, more scrutiny has been applied to the devices in the market. Some of the discoveries have concluded that even some of the currently available hospital grade oximeters perform poorly under certain conditions, particularly common in small children and sick patients. Many “conventional” pulse oximeters work under the assumption that only arterial blood is pulsatile. This is a sound assumption when the person/patient is not moving and has good perfusion, but fails to give an accurate reading when you need it most – when the patient is moving such as the case in small children and/or when the patient has poor perfusion due to cold hands or because the patient is very ill. Under these conditions, a conventional pulse oximeter is likely to display false (low or high) SpO2 readings and inaccurate pulse rates resulting in high incidence of false alarms. These false/inaccurate readings can also lead to clinical interventions that are not appropriate.
Masimo Signal Extraction Technology (SET®) has been designed to overcome the limitations of conventional pulse oximetry. Masimo SET® technology is trusted by care providers around the world – it is used to monitor more than 200 million patients each year, and has been shown in more than 100 independent and objective studies to outperform other pulse oximetry technologies, providing clinicians with unmatched sensitivity and specificity to make critical patient care decisions. This same tried and tested high quality technology (Masimo SET® pulse oximetry) is now available in the home for spot check and continuous measurement of oxygen saturations.
In addition to motion and low perfusion (cold hands or poor circulation), racial bias, where oxygen saturation readings are lower in dark skin patients, has been highlighted as an important issue and a possible factor in the increased mortality rate seen in ethnic patients who contracted COVID-19. This was a surprise to us at Masimo, as we have been calibrating our pulse oximeters using desaturation testing in both dark and light skinned subjects for over two decades. This recent focus on racial bias prompted us to re-examine our internal data and evaluate prospectively the accuracy, precision, and bias of the Masimo MightySat® with Masimo SET® pulse oximetry. In our analysis we used a rigorous study protocol and data interpretation paradigm. Our results indicated that the accuracy precision and bias between white and black patients monitored with Masimo MightySat® with Masimo SET® pulse oximetry was similar for all SaO2 readings and samples obtained during sequential desaturation in the range 100-70% oxygen saturation. Therefore, the recent retrospective reports of occult hypoxemia having racial bias do not apply to the Masimo MightySat® with Masimo SET® pulse oximetry. Patients, families and healthcare providers can rest assured that SpO2 values obtained from Masimo MightySat® with Masimo SET® pulse oximetry are accurate and free of racial bias. For more information please see www.masimo.co.uk/company/news/pulse-oximetry-racial-bias.

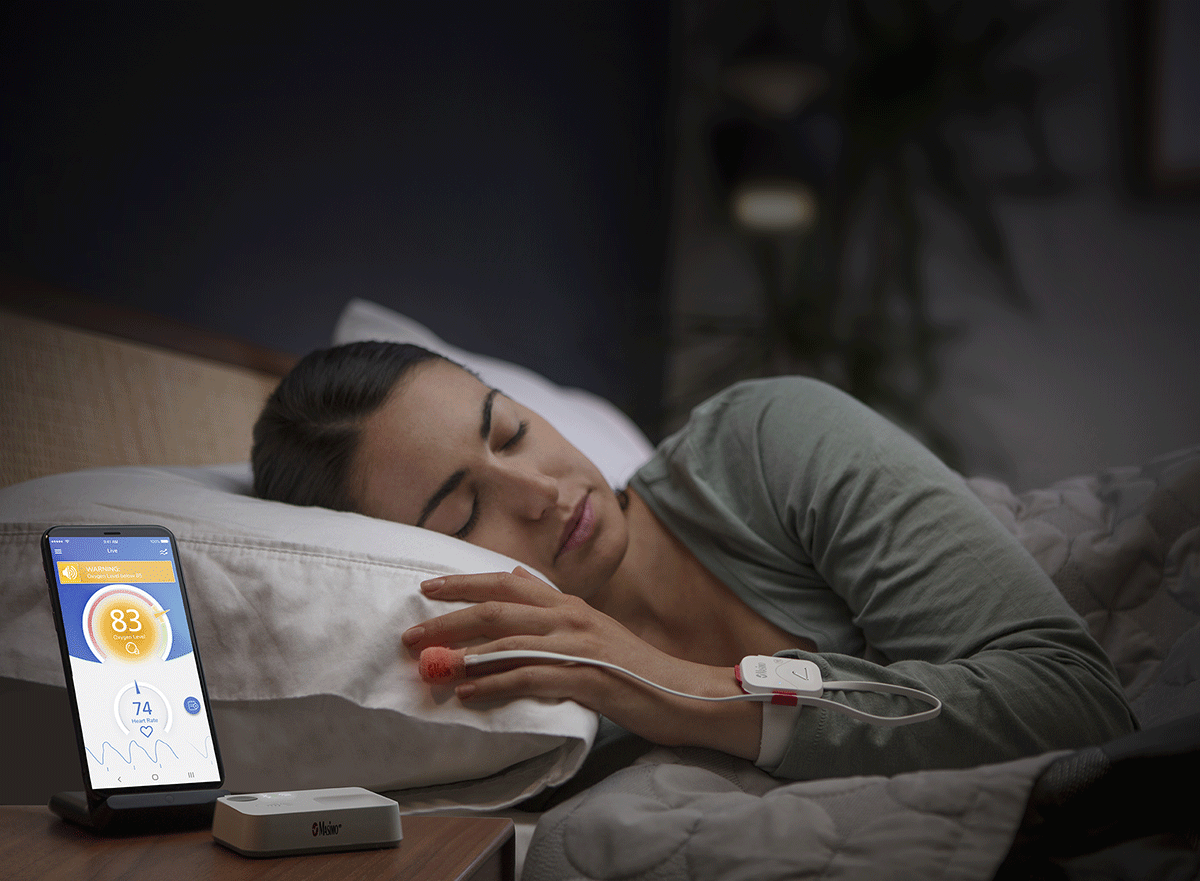
There is now evidence to suggest that continuous pulse oximetry monitoring is beneficial in detecting episodes of desaturation when patients are asleep – even at home, with hospital grade technology. Our Masimo SafetyNet® with Masimo SET® pulse oximetry is a remote monitoring solution that now provides the clinician with the ability to monitor patients while they are at home – thereby reducing hospital admissions without degrading care. The Masimo SafetyNet® Alert version of this remote monitoring solution allows “self-monitoring” by the individual, with alerts to wake the individual should oxygen saturations drop. Further sustained drops in saturations lead to text alerts being sent to a next of kin or designated health provider, and even a call to emergency services.


Dr. Basil Matta, Senior Medical Director for Masimo, is the immediate past Divisional Director for Musculoskeletal, Digestive Diseases, Major Trauma and Perioperative Care Medicine at Cambridge University Hospitals NHS, where he is a Consultant in Anaesthesia & Critical Care, and Affiliate Assistant Professor at the University of Cambridge.
Email: This email address is being protected from spambots. You need JavaScript enabled to view it.
The Existential challenge of Covid-19 and Climate change and it's impact on mental health - Dr Ishak Nadeem
 The two great challenges threatening humanity’s very existence are Covid-19 and Climate Change. Are there similarities between the two? If so what kind of linkages? Are there lessons to be learned from the handling of Covid-19 and its impact on mental health? Will these lessons be learnt and help us in dealing with the mental health impact of climate change?
The two great challenges threatening humanity’s very existence are Covid-19 and Climate Change. Are there similarities between the two? If so what kind of linkages? Are there lessons to be learned from the handling of Covid-19 and its impact on mental health? Will these lessons be learnt and help us in dealing with the mental health impact of climate change?
Warnings of science were unheeded for decades in both instances. Scientists had been warning about a pandemic since at-least 2007 and exhorting preventive action and science has been showcasing the precipitous loss of species, rising temperatures and loss of habitat for a number of decades and warning about the threat of Climate Change to both human health and existence. For decades we have watched the rising temperatures, the heatwaves, the increasing frequency of floods and wildfires, in denial of the fast-approaching catastrophe and our role in its causation. There is one crucial difference between the two. Covid-19 soon after its emergence in late 2019 spread like wild-fire and the effects were tangible. The scale of suffering and deaths was hard to ignore. Not so with climate change. It has not yet reached the threshold of tangibility apart for the small island nations!
The saga of suffering, death, the daily media briefings, the lockdowns, the race to develop a vaccine, the protests against loss of freedom and wearing of masks is well known and does not need repeating.
While the press coverage and media stories were highlighting the daily cases and death rates and focusing on saving lives and physical issues and rightly so, another picture in juxtaposition, was emerging in conversations with frontline healthcare workers and social media stories. A story of lockdown loneliness leading to low mood, depression and despair which was borne stoically by the elderly, a spate of theories about the “real cause” of Covid-19, conspiracy/alternative explanation theories with very little evidence spreading like wildfire on social media. Uncertain times are fertile ground for the growth of irrational ideas and instability.
But what has been the effect of two years of uncertainty, which incidentally continues? The fear, anxieties, depression, loneliness, and despair many of us felt both from listening to the stories of suffering and deaths, as well as from the lockdowns and curtailment of freedoms to socialise was nothing short of a collective Neurosis. And our response, Schizophrenic.
Race to develop a vaccine and the campaigns and marches by the Anti-Vaccine Lobby.
Masks and Social distancing vs the backlash against wearing masks and respecting personal space.
The freedom to roam free and the necessity of stopping the spread.
The sudden emergence of “expertise” amongst laypeople and the erosion of trust in experts and people in power.
And the neurosis continues and the Schizophrenia rages unabated with the emergence of yet more virulent strains and controversial reports about how the WHO has avoided naming the new strain as it clashes with the leader of a certain country.
We are not yet out of the woods and Covid-19 is still not conquered. Perhaps, we will never conquer it but come to terms with it and learn to live alongside it.
If that is the case with Covid-19, then what about the Climate Change Challenge?
Writing in the Bulletin of The Atomic Scientists in 2016 Eva Gifford and Robert Gifford commented, “In all of the coverage of climate change in the popular press, relatively little attention has been paid to one aspect: mental health. Rising seawaters, increasingly strong storms, and more ferocious droughts caused by climate change are not only devastating to physical infrastructure but also affect human beings in other ways as well: people lose their homes, their jobs, their family members, and their communities. Researchers have found that climate change can cause not only posttraumatic stress disorder (PTSD) from the trauma of displacement from extreme weather events such as Hurricane Katrina but also “pre-traumatic” stress disorder, or, moderate to extreme anxiety about a looming crisis.”
Nothing much has changed in the last five years. Not only does the coverage in the popular press of the effects of climate change on human health is still heavily weighted towards physical health effects and neglects the impact on mental health and human psychology, even the Environmental Audit Committee report “Our Planet Our Health” highlights physical health issues and barely mentions mental health problems, as follows.
“We are concerned that the NHS and the pharmaceutical industry is not sufficiently resourced to deal with these projected changes. Non-communicable diseases (NCDs) kill 41 million people each year, equivalent to 71 per cent of all deaths globally. We note that more people now die from non-communicable diseases than communicable diseases. We also note the recent stalling in life expectancy in the UK as a result of lifestyle changes with increased pressure for NHS resources. Public Health England should broaden its key performance indicators to include climate resilience and adaptation measures to tackle emerging diseases. These should include guidance to general practitioners and the pharmaceutical industry on Lyme disease, malaria, the zika virus and other emerging tropical diseases. We repeat our recommendation from our toxic chemicals report that Public Health England should introduce a comprehensive UK wide human and wildlife bio-monitoring scheme to measure the effects of toxic chemicals. A focus on lifestyle change means that it does not prioritise the impacts that wider economic and ecological changes will have on human health. Secondly, Public Health England must work across Government to advise local Government on the impacts of heat stress and protecting vulnerable communities, particularly the elderly, people living in care homes and those with kidney failure.”
 And as for mental health in this report –
And as for mental health in this report –
“Eco-anxiety, has emerged as a psychological disorder afflicting an increasing number of people concerned about the environmental crisis and suffering a sense of grief or loss. Eco-anxiety has been described by the American Psychological Association as “chronic fear of environmental doom”.
Our disregard of matters concerning the mind in contrast to our focus on the body is perhaps a reflection of the Cartesian duality which split the mind from the body and scientific materialism which gives primacy to matter and body. Can we deny the effects of bodily ailments on the mental health of a person? Can we brush under the carpet the effect of stress and other mental problems on immunity and other physical parameters? No!
But we do…
The BMA commenting on the autumn budget recently announced by the Chancellor, have highlighted.
- The announcement falls significantly short of the BMA’s call for investment of at least £4.6 billion a year by 2023/24.
- Mental health services for children and young adults – services that were already stretched and struggling, allocated nothing more than the inadequate £500m previously promised in March as part of the mental health recovery plan.
- Given the compounding effect of COVID-19 on the population’s mental health, with a 29% increase in the number of people referred to mental health services for their first suspected episode of psychosis between 2019 and 2021, urgent investment is needed in this area.
So what hope for “Parity Of Esteem”? It morphed into Mental Health Investment Standard.
As chair of a CCG in 2016 I heard quite a bit about the resolve to end stigmatisation of mental health and levelling up of services and resource allocation for mental health in proportion with the problem. Has it remained a pipe dream?
A cursory glance at the NHS Mental Health Dashboard for Q1 2021/22: NHS England » NHS mental health dashboard shows that all 106 CCGs are meeting their MHIS. Is this really true? And, only a few indicators show red dots on the dashboard. So is everything hunky dory?
Perhaps generalisations hide the gaps that granularity would reveal. Don’t we still hear the tales of interminable waits for assessments of children for autism and ADHD? Does the offer of a treatment within two weeks of contact in Psychosis really mean treatment has been started? Are there no loopholes that allow for obfuscation?
But then resources are finite and cannot keep pace with the demand on the NHS for providing the latest services. It might have been possible to provide universal healthcare when the NHS was set up. But medical practice has seen a sea change with technological advances, newer medicines and investigation techniques and it is impossible that any government can provide for all this while also focusing on education, defence etc. So the demands for more money for mental health services will fall on deaf ears.
So, what is the answer? Lockdown has shown us the noble side of humanity, the side that delivered food and shopping to housebound vulnerable individuals, the side that rose up to the challenge of lifting up our spirits and showing appreciation to the brave healthcare workers. A sense of community.
Even if we ignore the concept of quantum entanglement, can we ignore the interconnectedness of our globe as evidenced by the rapid spread of Corona Virus. Will the effects of Climate Change remain isolated to one area of the globe. Will the repercussions not spread throughout the globe? When we can have global corporations, global finance and global cultures, why not global communities? Cohesive, compassionate, caring global communities.
Likewise, we need a bigger role to be played by corporations and big business as part of their corporate social responsibilities.
A call for the Business and Corporate sector to assist in the response to face the climate change challenge at COP26 is very appropriate in these times.
So when the global governments leave gaps, be it with the resources for mental health or meeting the juggernaut of climate change, cooperative endeavours between businesses, government and communities are the solution. Only then can we survive these existential challenges.
Dr Ishak Nadeem was a GP Partner at Grovelands Medical Centre for 16 years. His career comprises of several chapters, after qualification and post graduate training in India he worked for about 6 years in Saudi Arabia, moving to UK in 1994 he trained to become a General Practitioner. Moving on to senior management he was on the Governing Body of South Reading CCG from 2012 till 2016, the last two years as Chair during which he gained experience of the challenges of commissioning and the demands on NHS. He has since moved on to a full time role as Occupational Physician with TPhealth providing occupational health services to the Atomic Weapons Establishment.
His other passions are photography, poetry and writing. He self published a book of pictures and poems - Rhythm Of Life, in aid of Dingleys Promise, and raised £1000.00.
Further he is the founder chairman of OneNature-CommonWealth CIO which aims to raise funds for projects which help build sustainable communities, protect environment and promote biodiversity throughout the Commonwealth. Visit their website at www.onenaturecommonwealth.org




 I have written and provided specialist pain management services at the Chelsea & Westminster Hospital for over 14 years now. Every Trust has a unique and differing inward population into their services and in the last decade I have dedicated myself to understanding our unique populations and writing / providing appropriate pain management services for all. More recently I have become engaged with the NWL CCG who are making a valiant attempt to think with a macro plan for pain services in this commissioning body. Watch this space for a new thoughtful, evenly accessible pain service across these boroughs.
I have written and provided specialist pain management services at the Chelsea & Westminster Hospital for over 14 years now. Every Trust has a unique and differing inward population into their services and in the last decade I have dedicated myself to understanding our unique populations and writing / providing appropriate pain management services for all. More recently I have become engaged with the NWL CCG who are making a valiant attempt to think with a macro plan for pain services in this commissioning body. Watch this space for a new thoughtful, evenly accessible pain service across these boroughs.



