



Hand-held devices (CardioChek®, Mission®) to smart phones (elemark™, 1drop™) for self-testing of blood cholesterol - J Bolodeoku MBBS, MSc, MBA, DPhil, FRCPath, FRSB
Self-monitoring or testing of blood cholesterol (SMBC) using hand-held devices or smartphones will be helpful in a number of distinct ways:
- Helping both the patient and clinician in being able to ascertain high or low levels of cholesterol and thereby make the necessary therapeutic adjustments.
- Providing the patients with the chance to more routinely detect or confirm whether their cholesterol levels are decreasing or increasing, without having to visit the lipid clinics.
- Allowing clinicians to track and monitor patients’ cholesterol levels remotely
- The SMBC devices will also provide patient education and disease management information in providing trends of their cholesterol and uric acid profiles and help motivate the patients.
There is a need for more real-world experience in the use of these devices in the management of these patients in the primary and outpatient settings to fully understand the true benefit and impact these devices in the management of patients undergoing therapeutic intervention. As self-monitoring of blood glucose is routine in the management of patients with diabetes mellitus, hopefully, self-monitoring of blood lipids will become routine in the management of patients undergoing treatment and monitoring of their lipid profiles.
Hand-Held devices (CardioChek® and Mission®)
Devices for measuring cholesterol for self-monitoring blood cholesterol devices such as the Mission®, BeneCheck™ Plus, CardioChek® PA, Veri-Q, 3in1 are on the market. They measure a number of lipid fractions (total cholesterol, triglycerides, high density lipoprotein, low density lipoprotein) and ratios on whole blood, plasma or serum collected from the finger or venous blood using reflectance or biosensor technology with single-use, disposable, dry reagent test strips, rotors or cassettes.
Hand-Held devices - Precision, accuracy, comparison, and biological variation
The precision (within and within-run precision) for the CardioCheK® PA, was 3.7% for total cholesterol and 6.2% for HDL-C for level 1 concentration and 3.6% for TC and 3.5% for HDL-C for level 2 concentration1. An evaluation by the UK NHS Purchasing and Supply Agency of the CardioChek® PA, showed for TC an imprecision of 12%, for HDL-cholesterol 22% and for TG 14%2. In a recent study, the precision of the CardioChek® PA was 5.4 – 8.3% for TC, 3.4% – 5.5% for HDL-C, 9.4% – 14.0% for LDL-cholesterol3. These values are marginally higher than the Cholesterol Reference Method Laboratory (CRMLN) cholesterol certification criteria for total cholesterol (TC) is < or = 3%, for and high density lipoprotein-cholesterol (HDL-C) is < or = 4% and for and low density lipoprotein-cholesterol (LDL-C) < or = 4% and HDL-C < or = 4% and the National Cholesterol Education Programme (NCEP) recommended precision performance criteria for laboratory TC is < or = 3% and HDL-C < or = 6%4,5.


Figure 1. Showing Mission® and CardioChek® hand-held devices for self-testing cholesterol.
The within person day to day variation in a healthy volunteer was assessed using the CardioChek®, for total cholesterol 9.4%, for triglyceride 23%, for HDL-cholesterol 7.0% and for LDL-cholesterol 14%6. The results were consistent with lipid concentrations described in the literature for healthy volunteers showing CV% ranges for total cholesterol of 2.5% - 10.9%, for HDL-cholesterol is 3.6% - 12.4%, for LDL-cholesterol 7.8% - 13.6% and for triglyceride 12.9% - 40.8%7-10.
When the CardioChek® PA was directly compared to a laboratory method using venous samples to determine device accuracy, the conclusion was that the device produced clinically equivalent values when compared to the same patients’ samples analysed in a reference laboratory and operated within industry accuracy standards1.
A comparative study was carried out to compare the lipid profile (total cholesterol, HDL-cholesterol and triglycerides) estimation between the Mission® ACON and CardioChek® PA, two cholesterol self-testing devices using finger prick (capillary) samples. Sixteen paired capillary blood samples were collected into microvettes (system for capillary blood collection) and the blood sample was pipetted using capillary transfer tubes and applied to the test devices on the Mission® ACON and CardioChek® PA devices respectively. The total cholesterol values estimated using the Mission® ACON device were generally higher than the values with CardioChek® PA ranging from -0.3 to + 10.0 mmol/L, with an average of +4.50 mmol/L. The HDL-cholesterol values estimated using the Mission® device were mostly higher than the values with CardioChek® PA ranging from - 3.1 to + 7.7 mmol/L, with an average of +1.12 mmol/L. The triglyceride values estimated using the Mission® device were mostly lower than the values with CardioChek® PA usually ranging from -19.6 to + 6.5 mmol/L, with an average of -0.2 mmol/L. In conclusion both the Mission® ACON and the CardioChek® PA lipid testing devices were easy to use and required a similar amount of blood. The analysis times were similar, and the total cholesterol and HDL-cholesterol estimates of the Mission® ACON device were, on average, 17% and 4% higher than the estimates from the CardioChek® PA. Whilst the triglycerides of the Mission® ACON device were on average 17% lower than the CardioChek® PA11.
Smart Phones (elemark™ and 1 drop)
Smart phones with their technological features (such as high-quality cameras, connectivity, and computational power) have increasingly led to their integration into a wide range of analytical sensing systems. Detection via smartphone is commonly based on various forms of optical measurements – including bright-field, colorimetric, luminescence, and/or fluorescence. The high resolution of the embedded complementary metal oxide semiconductor image sensor cameras enables high pixel density for optical monitoring, while the high computational power facilitates real-time image analysis because smart phone-based PoC platforms have been extensively reviewed in the past few years12.
elemark™
The elemark™ lipid check is a smart phone-based in vitro diagnostic device for rapid self-testing of lipid parameters. The elemark™ system includes the elemark™ analyser and the SD LipidoCare™ lipid test strip (figure 2)13.

Figure 2. Device components. (A) elemark™, (B) elemark™ lipid check, (C) elemark™ lipid check cholesterol test strip, (D) connection of the elemark™ lipid check to a compatible mobile device in the shown direction, (E) button is pushed to lock the elemark™ lipid check.
There was very high correlation for TC, HDL-cholesterol and TG results from the elemark™ device with those of laboratory method using the AU5800 Analyzer (Beckman Coulter Inc., IN, USA)13.
The precision of the elemark™ determined was 3.0% – 5.3% for TC, 4.3% – 6.2% for HDL-C and 5.5% – 14.4% for LDL-cholesterol3. These values were marginally higher that the Cholesterol Reference Method Laboratory (CRMLN) cholesterol certification criteria for total cholesterol (TC) is < or = 3%, for and high density lipoprotein-cholesterol (HDL-C) is < or = 4% and for and low density lipoprotein-cholesterol (LDL-C) < or = 4% and HDL-C < or = 4% and the National Cholesterol Education Programme (NCEP) recommended precision performance criteria for laboratory TC is < or = 3% and HDL-C < or = 6%4,5.
The within person day to day variation in a healthy volunteer was assessed using the elemark™ and its CV% fell within the CV% described in the literature: with a total cholesterol 5.0%, HDL-cholesterol 13%, LDL-cholesterol 13% and triglyceride 30%6. Consistent with lipid concentrations described in the literature for healthy volunteers showing CV% ranges for total cholesterol of 2.5% - 10.9%, for HDL-cholesterol is 3.6% - 12.4%, for LDL-cholesterol 7.8% - 13.6% and for triglyceride 12.9% - 40.8%7-10.
1drop™
1drop™ is an in-vitro diagnostic medical device that utilises the camera/flash function on a smartphone to measure different biomarkers of the body. With single membrane technology, plasma separation and enzyme reactions taking place simultaneously, so even just a small drop of blood can give a deep insight into one’s health. This device is paired with a smartphone app, allowing users to constantly check their results as well as explore measurements of newly added biomarkers.

Figure 3. Figure showing photograph Galaxy J3 with the specially designed smartphone cover and membrane containing dried reagents (1drop™ TC total cholesterol test cartridge)
Recently, we evaluated the performance (intra-individual variation, intra-assay precision and comparative data) of the 1drop™ smart phone in measuring total cholesterol. 1 drop™ Smartphone is a smart phone (figure 1) used to determine total cholesterol. In this pilot study, on a healthy volunteer, the 1 drop™ demonstrated a within in person variation CV% of total cholesterol of 7.3% and an intra-assay precision of 6%14. These values were marginally higher that the Cholesterol Reference Method Laboratory (CRMLN) cholesterol certification criteria for total cholesterol (TC) is < or = 3%, for and high density lipoprotein-cholesterol (HDL-C) is < or = 4% and for low density lipoprotein-cholesterol (LDL-C) < or = 4% and HDL-C < or = 4% and the National Cholesterol Education Programme (NCEP) recommended precision performance criteria for laboratory TC is < or = 3% and HDL-C < or = 6%4,5.
In the comparative study, the total cholesterol estimates of the 1 drop™ device were on average 6%, 13% and 23% more than the total cholesterol estimates of the Mission®, Prima 3in1 and CardioChek®, respectively14.
More recently, we estimated total cholesterol in 48 healthy blood donors using their finger prick (capillary samples). The estimated total cholesterol ranged between 2.8 – 8.9 mmol/L, with a mean of 4.8 mmol/L (data on file). This data was comparable to data seen in a normal population normal cholesterol range of 2.75 – 7.59 mmol/L, with a mean of 4.87 mmol/L (see figure 4). In addition, the intra-assay precision for total cholesterol determined was 5.9% (data on file). This value was marginally higher that the Cholesterol Reference Method Laboratory (CRMLN) cholesterol certification criteria for total cholesterol (TC) which is < or = 3%3,4

Figure 4. Showing histogram of total cholesterol estimated using traditional analyser method (upper half) and using 1 drop™ smart phone (lower half)
In conclusion, both the hand-held devices (Mission® and CardioChek®) and the smart phones (elemark™ and 1drop™) self-monitoring blood cholesterol devices correlate very well with the traditional laboratory cholesterol methods. Even though it appears that both the precision criteria (CRMLN and NCEP) are quite stringent for the portable hand-held and smart phone self-monitoring blood cholesterol devices, as all of the devices exceeded the expected analytical precision for TC of < or = 3%, for HDL-C of < or = 4%/6% and for LDL-C of LDL-C < or = 4%, they have a reasonable precision profile and they can be used very well by patients.
Real Life Usage
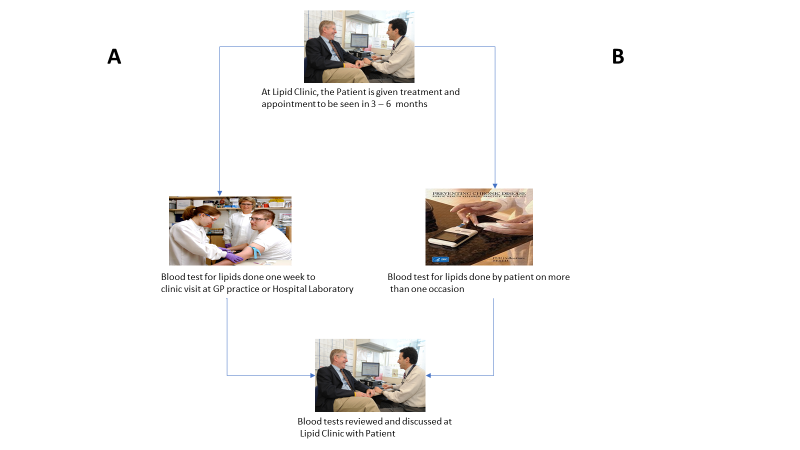
In the management of patients with hyperlipidaemia, it is the normal practice that after initiating pharmacological interventions such as statins, fibrates, bile acid sequestrants and more recently, PCSK9 inhibitors, the patients are expected to have a follow up laboratory test done at some appropriate time point. Patients will usually have these blood tests done at the local hospital laboratory or General Practice (GP) who would have the blood sample sent to the local hospital laboratory prior to their visit in order to have the cholesterol estimations ready for their out-patient visit. This way of conducting blood cholesterol measurements is not optimum as most clinicians are usually making a judgement call on one blood lipid profile estimation when the more optimum procedure will be to make the call after a review of more than one lipid profile. This would require the patient to attend the local hospital laboratory or General Practice (GP) at least more than once (route A in figure 1), this could be quite a bother to patients and therefore the question is, can portable hand-held self-monitoring of blood cholesterol (SMBC) (route B in figure 1) be of benefit in the management of these patients?
In a randomised study, investigating the value of home monitoring of lipids, one group of patients received the hand-held device (CardioChek® PA) and measured and reported their lipid levels for 6 months using a phone call (B), whilst the other group had their lipid levels measured in the usual way in the traditional laboratory setting (A).
The results showed that mean LDL-C decreased from 186 mg/dL (4.8 mmol/L) to 117 mg/dL (3.0 mmol/L) in the usual care group (A), whilst a similar reduction of LDL-C decrease from 162 mg/dL (4.2 mmol/L) to 105 mg/dL (2.7 mmol/L) was observed in the patients using the home monitoring (B), there was no significant difference between the mean changes. In addition, there was also no significant difference between the two groups with regards to mean changes in HDL-C and triglycerides15.
This review highlights that with the hand-held devices and smart phones that estimate total cholesterol, using the precision criteria (CRMLN and NCEP) for total cholesterol of < or = 3%, have a reasonable precision ranging between 3.0% - 7.3%. The estimates compared and correlated very well with the traditional laboratory cholesterol methods. Furthermore, they have been used in a home monitoring setting and compared well with the estimates obtained in the usual care in the traditional laboratory setting. More studies are required to demonstrate the benefit of self-testing of cholesterol in patients using these hand-held and smart phone devices.
References:
- Whitehead SJ, Ford C, Gama Rousseau. A combined laboratory and field evaluation of the Cholestech LDX and CardioChek® PA point of care testing lipid and glucose analysers. Ann Clin Biochem 2013; 51 (1) : 54–67
- Centre for Evidence Based Purchasing. CEO catalogue search. London. Department of Health http://www.healthcheck.nhs.uk/document.php?o=11
- Bolodeoku J, Pinkney S, Imprecision evaluation of self-monitoring of blood cholesterol (SMBC) handheld point of care testing devices: elemark™ and CardioChek® PA. Ann Clin Lab Res Vol. 7 No. 1: 290
- National Cholesterol Education Program Laboratory Standardization Panel. Current status of blood cholesterol measurement in clinical laboratories in the US. Clin Chem 1988; 34: 193-201
- National Cholesterol Education Program Laboratory Standardization Panel. Recommendations for measurement of high-density lipoprotein cholesterol; executive summary. Clin Chem 1995; 41 : 1427-1433
- Bolodeoku J. Biological Variation of Self-Monitoring of Blood Cholesterol (SMBC) Using Portable Handheld Point of Care Testing Devices: 3in1, Cardio Chek PA and Elemark™. Curr Trends Med Diagn Meth 2018: CTMDM-106. DOI: 10.29011/ CTMDM-106.100006
- Hammond J, Wentz P, Statland BE, Phillips JC, Winkel P. Daily variation of lipids and hormones in sera of healthy subjects. Clinica Chimica Acta 1976; 73 (2) : 347 – 352
- Demacker PNM, Schade RWB, Jansen RTP, Laar AV. Intra-individual variation of serum cholesterol triglycerides and high-density lipoprotein cholesterol in normal humans. Atherosclerosis 1982; 45 (3) : 259 – 266
- Gidding SS, Stone NJ, Bookstein LC, Laskarzewski PM, Stein EA. Month to month variability of lipids, lipoproteins and apolipoproteins and the impact of acute infection in adolescents. The Journal of Pediatrics 1998; 133 (2) : 242 – 246
- Bookstein L, Gidding SS, Donovan M, Smith FA. Day to day variability of serum cholesterol, triglyceride and high-density lipoprotein cholesterol levels. Arch Intern Med 1990; 150 (8) : 1653 – 1657
- Clark S, Bolodeoku J. Self-cholesterol measuring devices Mission® and CardioChek®: total cholesterol, triglycerides. High density lipoprotein (HDL) – cholesterol estimations in whole blood samples. Biomed J Sci & Tech Res 35 (4) – 2021. BJSTR.MS.ID.005735
- Arumugam S, Colburn DAM, Sia SK. Biosensors for Personal Mobile Health: A System Architecture Perspective. Adv Mater Technol. 2020 Mar;5(3):1900720. doi: 10.1002/admt.201900720. Epub 2019 Nov 20. PMID: 33043127; PMCID: PMC7546526.
- Yun K, Lee J, Choi J, Song I-U, Chung Y-A. Smartphone based point of care lipid blood test performance evaluation compared with a clinical diagnostic laboratory method. Appl Sci. 2019, 9, 334; doi:103390/app9163334
- Bolodeoku J, Clark S, Anyaeche C. Self-monitoring of blood cholesterol 9SMBC) using the total cholesterol testing cartridge on the 1 drop™ smartphone. Biomed J Sci & Tech Res 29 (2)-2020 BJSTR.MS.ID.004760
- Alkouli MA, Carry BJ, Jarrett H, Sirna SJ. Management of hypercholesterolaemia utilizing a home lipid monitoring system; preliminary findings. J Clin Lipid 2013; 7 (3) : 254 – 255
Content provided by John Bolodeoku
MBBS, MSc, MBA, DPhil, FRCPath, FRSB
Address:
Lipid Clinic, Department of Cardiology
Basingstoke & North Hampshire Hospital
Aldermaston Road, Basingstoke
Hampshire, United Kingdom
RG24 9NA
This email address is being protected from spambots. You need JavaScript enabled to view it.
Tel No. +44 7765401135





