


Why Treating Erectile Dysfunction and the use of Vacuum Erection Devices are important to Men’s Health - iMEDicare
 Intimacy is one of the great joys and pleasures of life – alongside food, travel, arts and culture, especially in the context of a long term loving committed relationship – often it is one of the important glues that holds a relationship together. Most people will agree with this synopsis. Imagine your life without intimacy. Obviously, there is a huge social and psychological impact to the individual and partner in having ED. Studies exist that demonstrate psychological impact and increased morbidity in afflicted patients.Intimacy is one of the great joys and pleasures of life – alongside food, travel, arts and culture, especially in the context of a long term loving committed relationship – often it is one of the important glues that holds a relationship together. Most people will agree with this synopsis. Imagine your life without intimacy. Obviously, there is a huge social and psychological impact to the individual and partner in having ED. Studies exist that demonstrate psychological impact and increased morbidity in afflicted patients.
Intimacy is one of the great joys and pleasures of life – alongside food, travel, arts and culture, especially in the context of a long term loving committed relationship – often it is one of the important glues that holds a relationship together. Most people will agree with this synopsis. Imagine your life without intimacy. Obviously, there is a huge social and psychological impact to the individual and partner in having ED. Studies exist that demonstrate psychological impact and increased morbidity in afflicted patients.Intimacy is one of the great joys and pleasures of life – alongside food, travel, arts and culture, especially in the context of a long term loving committed relationship – often it is one of the important glues that holds a relationship together. Most people will agree with this synopsis. Imagine your life without intimacy. Obviously, there is a huge social and psychological impact to the individual and partner in having ED. Studies exist that demonstrate psychological impact and increased morbidity in afflicted patients.
What is erectile disfunction (ED)?
ED is the persistent inability to attain and/or maintain an erection sufficient for satisfactory sexual performance and is caused by various vascular, neuronal, hormonal and metabolic factors, mediated by endothelial and smooth-muscle dysfunction. Although most causes of ED are physical, some are due to psychosexual issues; nevertheless, all patients with ED should have a history, examination and investigations performed, even if a psychological cause is suspected. ED is a cardiovascular (CV) risk factor, posing a risk equivalent to that of current, moderate smoking. ED is also an important marker for future CV events, with symptoms occurring some 3–5 years before an event (1,2). The physical and psychosocial effects of ED can significantly affect the quality of life of patients and their partners (3).
Who is at risk?
The risk factors for ED are similar to those for cardiovascular disease (CVD) (1,2): Older age / Sedentary lifestyle / Obesity / Dyslipidaemia / Metabolic syndrome / Diabetes and Smoking among others.
Depression and EDMany studies have shown a consistent bi-directional association between ED and symptoms of depression (4) but a recent 8-year study found that depression at baseline failed to predict incident ED, suggesting that depression is a likely consequence of ED (5). The Caerphilly Cohort Study (BMJ 1997) - 50% reduction in cardiac death with 3 or more orgasms per week (calculated to equate to an extra 4.28 years of life). Acute Stress and Performance Anxiety ED can be triggered or maintained by performance anxiety, a process involving interplay among the cognitive, affective, behavioural, and physiological responses throughout a sexual situation. It can be triggered by any sexual stimulus that a man associates with his sexual inadequacy (6). Continuous erectile failure can lead to sexual avoidance and decreased sexual arousal. There is no doubt that ED can lead to relationship breakdown – and in many cases – divorce with all the detrimental mental health trappings for all involved including the children. We have established that treating ED is important.
Why do Vacuum Erection Devices (VED’s) matter?
In a nutshell – because they are very effective, low risk and low cost. There are over 50 published VED efficacy studies since their inception as an FDA approved product in 1982 (some of these studies are old but were rigorously applied and measure very observable outcomes). The cross category efficacy of medical grade VED’s is approx. 90%, (See table 1 below) which reflects the fact that approximately 10% of men are either contra-indicated or lack the dexterity to manage a VED. However 90% - with correct technical tuition will be successful without any restriction of frequency of use either for intimacy or therapeutic application.
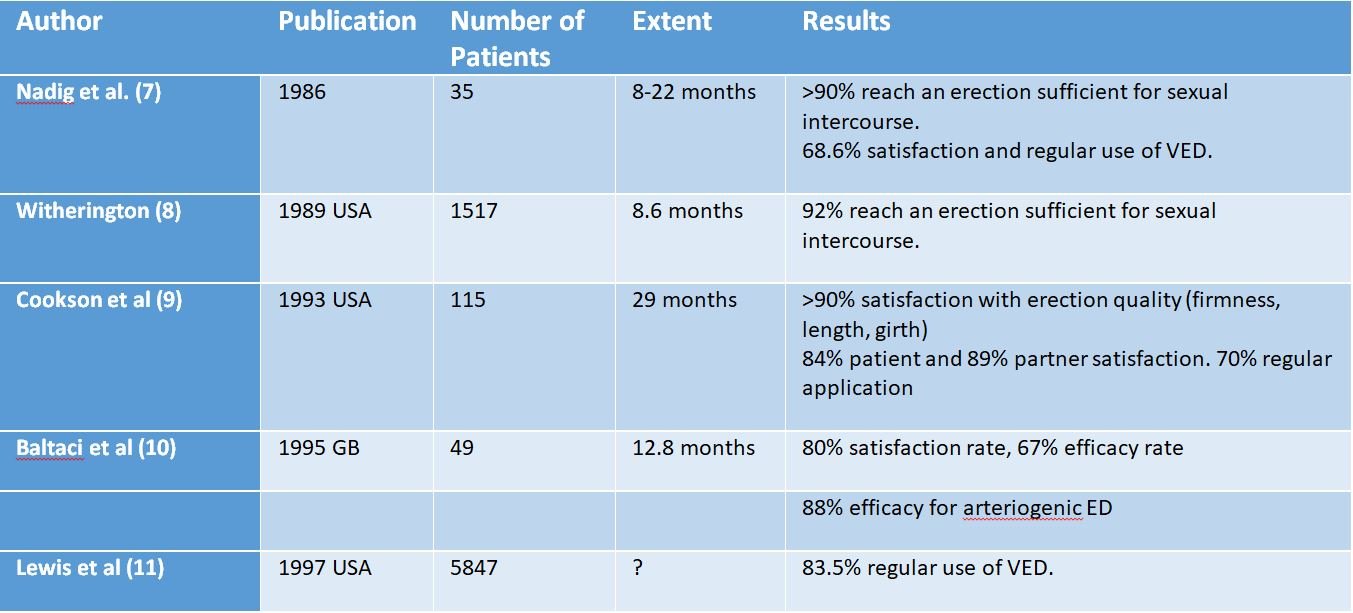
Table 1: Outcomes of VED Efficacy Studies
The British Society for Sexual Medicine Guidelines on the Management of Erectile Dysfunction in Men – 2017 (12) recommends use of VED’s as a first line treatment response if lifestyle modification and PDE5 medication has not proved effective. They reference VED’s as being “Highly effective, regardless of ED aetiology” (11,13,14).They can also be “a useful adjunct to PDE5 /injection therapy post-RP, and to salvage treatment failures” (15). VED therapeutic application post-prostatectomy is also well established and supported by the BSSM / MacMillan / PCUK (16) (Regular V.E.D. usage equates to a penile gym effect – oxygenation and mechano-receptor stimulation prevents dis-use atrophy (cavernosal fibrosis) and reverses penile shrinkage: See table 2 below.
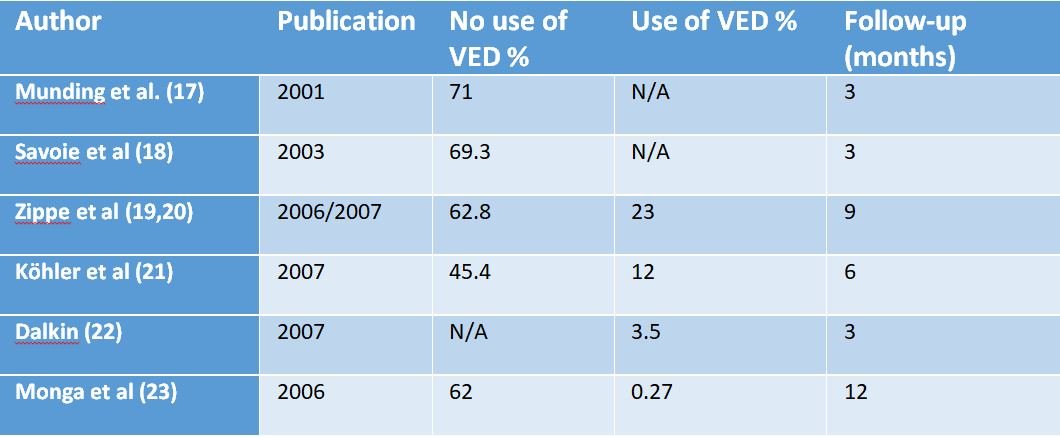
Table 2: Reduction in Penis Size (% No) after radical prostatectomy with and without the use of a vacuum erection system
It should also be recalled that a significant co-hort of men will not respond adequately to pharmacological Tx options for ED, will suffer adverse reactions or will be contra-indicated (24-31).
The SOMAerect VED brand, from iMEDicare Ltd (www.MyPelvicHealth.co.uk), is the most popular in the UK clinical context and comes in 5 different cylinder size options (Size to Fit concept ), manual and battery operated pump heads, 5 erection maintenance ring types (each in variable sizes) and is warrantied for 5 years for a mere cost of £167.32 on NHS prescription. If used 3 times per week for sexual purposes, that equates to a per usage cost of 21p (52 x 3 x 5 = 780 applications) over the 5 years. As a company, iMEDicare’s regional Tier 3 MIA credentialled reps will provide 1 to 1 patient training either in an NHS Hospital outpatient or home visit / tele-video context to ensure correct application of technique and customization of their system. Reliability and consistency are key at boosting self-confidence and ensuring longer term patient user compliance and satisfaction rates – assisted enormously by this 1 to 1 training (32). The goal is to ensure investment in SOMAerect is justified and warranted for every single patient.
So what is the problem?
The problem is that some CCG’s have elected to restrict the availability of VED’s on local formularies and in some cases removed VED’s from their formularies altogether. This creates a post-code lottery – with significant regional variations and disparity in quality and scope of ED service provision. This has not gone unnoticed and prominent organizations like Prostate Cancer U.K. have found that 76% of men who are treated for prostate cancer experience erectile dysfunction (ED), yet only 30% told them their ED treatment met their needs (33). PCUK has been contacting NHS Trusts and CCG’s in the worst performing areas and asking what they are doing to meet the needs of prostate cancer patients. The aim is to understand the barriers to providing good provision so they can help to find ways to assist.
Wider context
Many men cannot afford to buy a medical grade vacuum erection device privately – the price of which to buy privately is rising rapidly amidst an economy straining under the impact of C19 and an uncertain future Brexit outcome. As highlighted previously, in many cases a pharmaceutical alternative is either not sufficiently effective, brings unacceptable adverse effects or is simply contra-indicated. We’ve also seen that in some cases the cost of not treating ED to the individual and to society as a whole can potentially exceed the modest cost of treatment (34,35). It begs the question as to how these disparities in treatment provision can exist? Of course CCG’s are permitted to make local decisions on how to prioritise precious healthcare funding, however it is the authors view that these decisions are not always made with full consideration of the bigger impact on the men’s health agenda.
Ideally, long-term costs and utility data should be taken into consideration when determining the best treatment options for a patient with ED (36). As costs associated with switches related to successive treatment failures can be high, treatment considerations should, therefore, focus on achieving long term patient satisfaction. The patient’s preferred treatment choice, using goal-directed therapy during the initial consultation and evaluation visit, should be used (37). If we consider the German experience – pumps are universally prescribed and available to all men with either state health insurance or adequate private Health insurance. Germany must also carefully rationalise healthcare expenditure – however it would appear that in Germany, Men’s Health remains a front and centre societal and healthcare consideration. The good Men (and Women) of Britain will laud a similar consideration in this context.
References
- Thompson IM et al. Erectile dysfunction and subsequent cardiovascular disease. JAMA 2005;294:2996-3002.
- Vlachopoulos CV et al. Prediction of cardiovascular events and all-cause mortality with erectile dysfunction: a systematic review and meta-analysis of cohort studies. Circ Cardiovasc Qual Outcomes 2013;6:99-109.
- Feldman HA et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 1994;151:54-61.
- Atlantis E, Sullivan T. Bidirectional association between depression and sexual dysfunction: a systematic review and meta-analysis. J Sex Med 2012;9:1497-1507.
- Araujo AB, Durante R, Feldman HA, et al. The relationship between depressive symptoms and male erectile dysfunction: cross-sectional results from the Massachusetts male aging study. Psychosom Med 1998;60:458-465.
- Kirana P-S, Porst H. Erectile dysfunction in EFS and European Society for Sexual Medicine syllabus in clinical sexology. 2013 p. 598e635. 2013 MEDIX. ISBN/EAN 978-94-91487-10-1.
- Nadig PW, Ware JC, Blumoff R. Noninvasive device to produce and maintain erection-like state. Urology 1986; 27: 126–131.
- Witherington R. Vacuum constriction device for management of erectile dysfunction. J Urol 1989; 141: 320–322.
- Cookson MS, Nadig PW. Long term results with vacuum constriction device. J Urol 1993; 149: 290–294.
- Baltaci S, Aydos K, Kosar A, Anafarta K. Treating erectile dysfunction with vacuum tumescence device: a retrospective analysis of acceptance and satisfaction. Br J Urol 1995; 76: 757–760.
- Lewis RW, Witherington R. External vacuum therapy for erectile dysfunction: use and results. World J Urol 1997; 15: 78–82.
- Hackett G et al. British Society for Sexual Medicine Guidelines on the Management of Erectile Dysfunction in Men – 2017. J Sex Med 2018;15:430-57.
- Levine LA et al. Vacuum constriction and external erection devices in erectile dysfunction. Urol Clin North Am 2001;28:335-41.
- Dutta TC et al. Vacuum constriction devices for erectile dysfunction: a long-term, prospective study of patients with mild, moderate, and severe dysfunction. Urology 1999; 54:891-3.
- 28. Brock G et al. Safety and efficacy of vardenafil for the treatment of men with erectile dysfunction after radical retropubic prostatectomy. J Urol 2003;170:1278-83.
- International Journal of Clinical Practice Published by John Wiley & Sons Ltd Int J Clin Pract doi: 10.1111/ijcp.12338
- Munding M, Wessels H, Dalkin B: Pilot study of changes in stretched penile length 3 months after radical retropubic prostatectomy. Urology 2001, 58:567–569.
- Savoie M, Kim S, Soloway M: A prospective study measuring penile length in men treated with radical prostatectomy for prostrate cancer. J Urol 2003, 169:1462–1464.
- Zippe C, Nandipati K, Agarwal A, Raina R: Sexual dysfunction after pelvic surgery. Int J Impot Res 2006, 18:1–18.
- Zippe C, Pahlajani G: Penile rehabilitation following radical prostatectomy: role of early intervention and chronic therapy. Urol Clin North Am 2007, 34:601–618.
- Köhler T, Pedro R, Hendlin K: A pilot study of early use of vacuum erection device after radical retropubic prostatectomy. BJU 2007, 100, 858–862.
- Dalkin B: Preservation of penile length after radical prostatectomy (RP). Early intervention with a vacuum erection device (VED) [abstract]. Presented at the Society of Urologic Oncology Meeting. Anaheim, CA; May 19–14, 2007.
- Monga M, Köhler T, Hendlin K: Early use of vacuum constriction device following radical retropubic prostatectomy: a randomized clinical trial. Urology 2006, 68:262.
- Cialis 10 mg film coated tablet SmPC. Eli Lilly and Company. March 2017.
- Levitra 10 mg orodispersible tablets SmPC. Bayer PLC. December 2017.
- Viagra 100 mg film coated tablets SmPC. Pfizer Ltd. June 2016.
- Spedra 100 mg tablets SmPC. A. Menarini Farmaceutica Internazionale SRL. November 2017.
- Caverject 10 μg powder for solution for injection SmPC. Pfizer Ltd. March 2017.
- Invicorp 25 μg/2 mg solution for injection SmPC. Evolan Pharma AB. September 2017.
- MUSE 1000 μg urethral stick SmPC. MEDA Pharmaceuticals. December 2013.
- Vitaros 3 mg/g cream SmPC. Ferring Pharmaceuticals Ltd. October 2017.
- Int J Impot Res - Efficacy of vacuum erectile devices (VEDs) after radical prostatectomy- the initial Irish experience of a dedicated VED clinic
- (https://prostatecanceruk.org/about-us/projects-and-policies/erectile-dysfunction)
- A cost-utility analysis of phosphodiesterase type 5 inhibitors in the treatment of erectile dysfunction In the setting of recently introduced severity classifications and willingness-to-pay thresholds - Hansen, Svenn Alexander – Masters Thesis.
- Pharmacoeconomics - 1999 Dec;16(6):699-709. doi: 10.2165/00019053-199916060-00008. Annual cost of erectile dysfunction to UK Society - J M Plumb 1, J F Guest
- Cost-utility analysis comparing surgical and nonsurgical interventions in the treatment of erectile dysfunction- Orr Shauly, Daniel J. Gould & Ketan M. Patel . European Journal of Plastic Surgery volume 43, pages613–620(2020)
- Economic cost of male erectile dysfunction using a decision analytic model: for a hypothetical managed-care plan of 100,000 members. Tan Howard - Health Outcomes Research Design Consultants LLC, Dover, Delaware, USA
![]()
Content provided by iMEDicare.For more information please visit www.mypelvichealth.co.uk.

 After World War One, the role of women in British society changed forever. There are people out there who think that we ought to thank the Suffragettes for women’s suffrage. They’re wrong, in comparison to Kaiser Wilhelm II their role was quite minor. Only the pressures and opportunities provided by the world’s first total war compelled government and society to integrate women into the work force on a large scale.
After World War One, the role of women in British society changed forever. There are people out there who think that we ought to thank the Suffragettes for women’s suffrage. They’re wrong, in comparison to Kaiser Wilhelm II their role was quite minor. Only the pressures and opportunities provided by the world’s first total war compelled government and society to integrate women into the work force on a large scale.