Benefits of softening water for eczema sufferers - Kinetico
With a true heritage in the water treatment industry and more than 40 years of experience, Kinetico has used its knowledge and expertise to offer customers a wide range of products that provide different water treatment solutions.With a true heritage in the water treatment industry and more than 40 years of experience, Kinetico has used its knowledge and expertise to offer customers a wide range of products that provide different water treatment solutions.
Kinetico can provide a ‘whole house’ solution to treat the water in your home whether that’s a softener to prevent limescale build up, or a filtration system to take out the impurities from your drinking water. Many of our customers have both products installed in their home ensuring the water they bathe with, drink with, cook with and clean with is, simply...the best!
 We have all heard of hard water, but what exactly is it?
We have all heard of hard water, but what exactly is it?
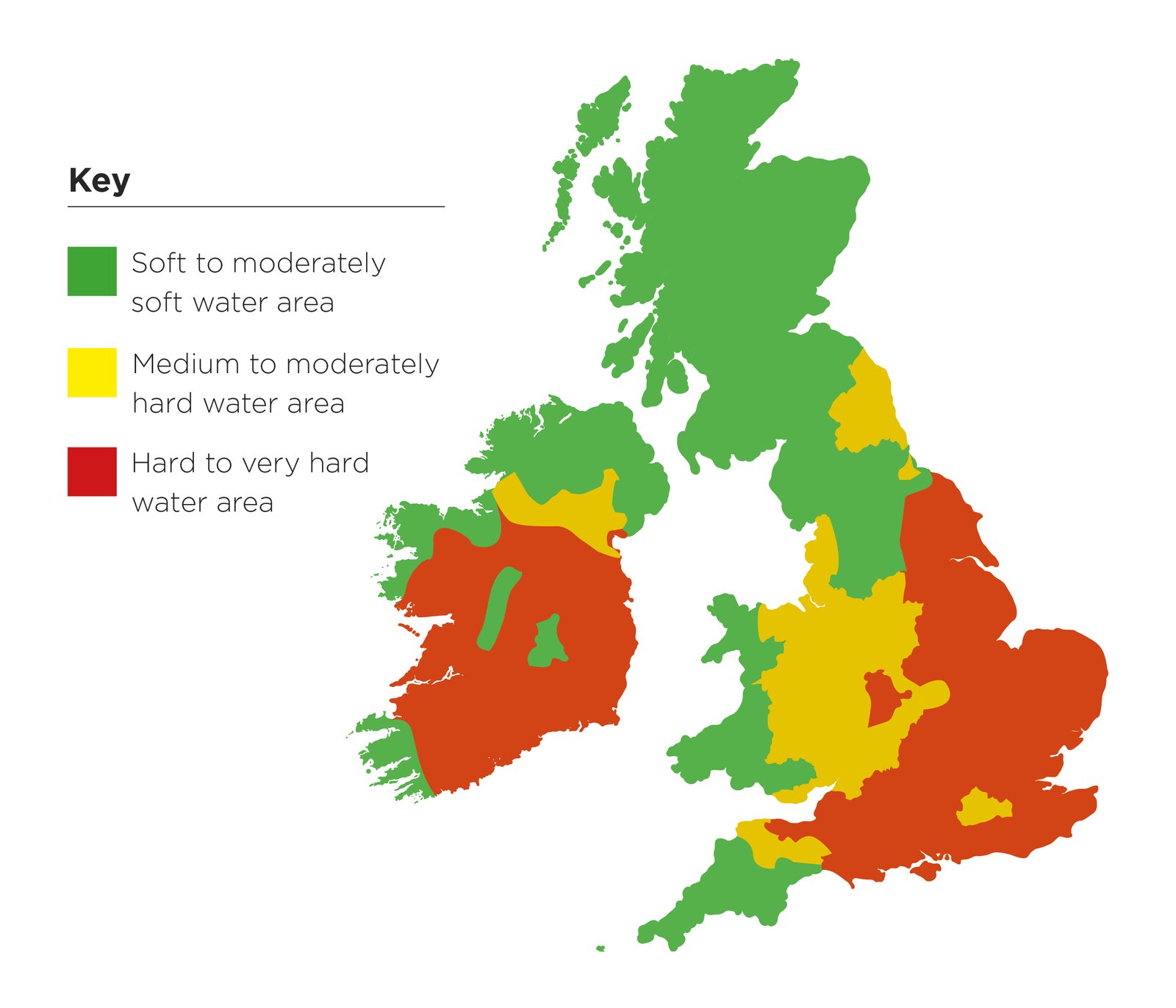
Whether your water supply consists of hard or soft water is determined by the geology of the ground that the rain in your region falls upon. Pure rainwater is naturally soft, but the chalk and limestone regions of the south and east of England surrender calcium and magnesium into the natural water supply to create hard water.
The granite areas of the north and west do not contain the same minerals and so the water remains ‘soft’. And with the development of water distribution networks, some parts of the UK which have historically been soft water areas, are now beginning to experience hard water.
As hard water is heated (e.g. in washing machines, showers, kettles etc), the Calcium and Magnesium separate out and form a crust on surfaces they come into contact with. This is what we know as limescale.The scale contained in hard water can cause damage and expense in the home...
Limescale build-up in heating systems causes a loss in heating efficiency, wasting energy. Showers, washing machines and immersion heaters become damaged and inefficient more quickly. Limescale quickly builds up on taps, sinks and other fittings becoming unsightly and making cleaning difficult.
Hard water can aggravate skin conditions such as eczema.
Kinetico water softeners revert hard water back to the natural composition of soft water, removing the substances that cause the damaging limescale build-ups throughout your home.
Kinetico commissioned talkeczema – one of the UK’s largest eczema support groups - to conduct an independent product trial and survey.
A Kinetico water softener was installed in the homes of selected talkeczema members for a 3 month period. The participants completed a questionnaire at the end of each month.
Comments from participants:
“Since using a water softener her skin does feel smoother and I have to use less cream. Also at the moment less reaction when in contact with the water.”
“Even my husband has said how moisturized his skin feels after showering. I have even managed to reduce the amount of emollient that I apply each day to my daughter.”
“I cannot believe the difference the softener has made, I am no longer getting dry flaky patches on my face. And there is the added bonus of not having to use so much detergent in my wash etc, so that’s got to better for my skin too.”
Commenting on these results, Julie Van Onselen, Independent Dermatology Nurse, said,
“These results show the people who participated in this survey felt the addition of a water softener benefitted and improved the severity of their eczema. The most positive result is that people with eczema felt their skin was less itchy and smoother. The vicious scratch-itch cycle is often the hardest symptom to deal with, dry skin is itchy skin and itchy skin is scratched, which leads to damage and often a “flare-up” of eczema.”
Therefore, if skin is less itchy, scratching and skin damage will reduce and eczema “flares” will reduce.
Kinetico has helped many eczema sufferers over the years
Dylan Flanagan-Crawford, aged 3 years.
Dylan used to suffer very badly from eczema. It was so terrible he had to wear special suits 24 hours a day and his skin was raw from his constant scratching. Despite being prescribed many different creams by his GP nothing seemed to work.
After some online research, Dylan’s mother contacted Kinetico and had a water softener installed. The transformation was remarkable. Within a few weeks Dylan’s eczema dramatically improved - and eventually vanished. Now he leads an active life, loves playing football and doesn’t have to worry about bathtime.
“My son has had eczema since he was 4 weeks old - very, very severe. We had our Kinetico water softener installed about 18 months ago. He’s a different child now - it’s a miracle! And we know it’s down to the softener as we went without it for 2 weeks when we were flooded.
His skin became dry, cracked, sore and the itch so intense he was reliving the nightmare again. Why don’t specialists tell sufferers about the benefits these devices can have? It truly is a light at the end of what can seem a very dark tunnel.” Mrs K Ward, Worcestershire
People with eczema might find their skin improves when they install a water softener or move to a soft water region.
This is because hard water contains high levels of calcium and magnesium, which can potentially irritate the skin.
Another reason is that households in hard water areas tend to use more soap and detergent when washing clothes and bathing - products we know inflame the skin of eczema sufferers.
Water softeners have an ‘ion exchange’ system which removes the calcium and magnesium salts from the water, thus completely eliminating the hardness.
How does an ion-exchange water softener work?
Water hardness is mainly due to calcium (and sometimes magnesium) in the water supply. To soften the water an ‘ion-exchange’ softener removes the calcium and magnesium almost completely.
The softener contains tiny beads of ‘ion-exchange resin’. These beads of resin are preloaded with sodium and as the water passes through the beads, the calcium and magnesium in the water supply swap places with the sodium. Calcium and magnesium remain on the resin, while sodium goes into the softened water. As sodium does not cause hardness, the water becomes softened.
Other water softener benefits
Softened water has all the benefits of naturally soft water, including:
Smoother skin and silkier hair.
Clothes feeling softer and looking brighter.
Preventing limescale in water heaters, central heating system, etc.
Saving fuel by increasing boiler efficiency.
Reducing boiler maintenance costs.
Reducing soap and detergent usage and cost.
Reducing scum on sanitary-ware.
Reducing cleaning frequency.
Reducing environmental impact by lowering carbon dioxide emissions and soap/detergent discharge to waste.

Kinetico are a world-leading manufacturer of high quality domestic & commercial water treatment products. For more information please visit www.kinetico.co.uk
Eating healthily: think it's hard to put into practice? Think again! - Action on Salt
 This means eating a wide variety of foods in the right proportions to ensure that you get all the nutrients you need, in the right amounts for optimal health and to maintain a healthy body weight. Eating too little or too much of the wrong types of food and drink can cause a multitude of problems - from nutrient deficiencies to chronic diseases like type 2 diabetes, coronary heart disease and cancer. Currently in the UK, over two thirds of adults and one third of children aged 10-11 years are overweight or obese; it’s clear that people are getting the balance wrong. types of food and drink can cause a multitude of problems - from nutrient deficiencies to chronic diseases like type 2 diabetes, coronary heart disease and cancer. Currently in the UK, over two thirds of adults and one third of children aged 10-11 years are overweight or obese; it’s clear that people are getting the balance wrong.
This means eating a wide variety of foods in the right proportions to ensure that you get all the nutrients you need, in the right amounts for optimal health and to maintain a healthy body weight. Eating too little or too much of the wrong types of food and drink can cause a multitude of problems - from nutrient deficiencies to chronic diseases like type 2 diabetes, coronary heart disease and cancer. Currently in the UK, over two thirds of adults and one third of children aged 10-11 years are overweight or obese; it’s clear that people are getting the balance wrong. types of food and drink can cause a multitude of problems - from nutrient deficiencies to chronic diseases like type 2 diabetes, coronary heart disease and cancer. Currently in the UK, over two thirds of adults and one third of children aged 10-11 years are overweight or obese; it’s clear that people are getting the balance wrong.
In 2016, Public Health England (PHE) launched a new healthy eating model for the UK called the Eatwell Guide, which shows the amounts and types of foods we should be eating (as well as those to consume less often and in small amounts), in order to have a healthy, balanced diet.
In essence, the focus is on eating whole fruits and vegetables, high fibre starchy carbohydrates and cutting down on fat, salt and sugar. Here we explain what it means in terms of the foods and drinks we buy and consume on a regular basis, along with a few tips to help.

Less fat, sugar and salt
Fat provides calories, and too many calories can lead to weight gain and obesity which increases the risk of diseases like coronary heart disease and type 2 diabetes. We only need a small amount of fat in our diets, and this should be unsaturated fat from plant sources (i.e. vegetable or olive oil) as this is healthier than saturated fat found in animal products like butter. Too much saturated fat increases blood cholesterol, which also increases the risk of coronary heart disease.
If you’re cooking with fat, it’s better to use oil instead of hard fats like butter, goose fat or lard. However, all oils and spreads are high in fat and contain a lot of calories, so they should be used and consumed in small amounts. Like fat, sugar also contains calories. Regularly consuming foods and drinks high in sugar (like biscuits, cakes, chocolate, ice cream, sweets and soft drinks) increases your risk of obesity and tooth decay.
As a nation we are consuming around 2-3 times more sugar every day than what is recommended, and so cutting back on these types of products is important to avoid damaging our health and teeth. These foods are not an essential part of the diet; they should only be consumed in small amounts and not every day.
Remember sugar is also hidden in foods that we might not expect to find it in - including those that don’t necessarily taste sweet - like soups, sauces and ready meals.
Eating too much salt raises blood pressure, which increases the risk of heart attacks and strokes. 75% of the salt we eat is already present in the food we buy, including foods that don’t necessarily taste salty, like bread and breakfast cereals. In the last 15 years the UK has led the way with a successful salt reduction programme that has seen the amount of salt added to food by manufacturers lowered, with products now containing around 20-40% less salt.
However, there is still more that can be done, as our salt intakes are still too high (about 8g per day on average compared to the recommended maximum daily limit of 6g). That’s why it’s important to check the label and compare products, choose those with less salt and avoid adding salt during cooking or at the table.
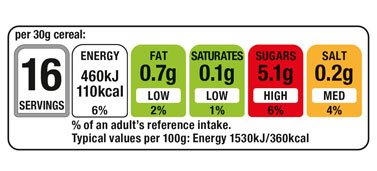
Lots of pre-packaged foods and drinks have a colour coded nutrition label on pack which shows you the amount of energy, fat, saturated fat (referred to as ‘saturates’), sugars and salt in a serving of that product. It is better to go for products with fewer reds and more ambers and greens, as these indicate healthier choices.
 Eat more fruit and vegetables - at least 5 A DAY
Eat more fruit and vegetables - at least 5 A DAY
Fruit and vegetables provide a range of different nutrients and fibre and we should aim to eat at least 5 portions a day (1 portion =80g). It’s better to eat the fruit or vegetable whole, rather than drink it in juiced form. Fruit juices and smoothies don’t provide the same nutritional benefits as the whole fruit or vegetable, and they contain free sugars which we need to eat less of.
Swap canned fruit in syrup for fruit in juice and choose canned veg in water with no adder sugar or salt. Avoid adding sugar, salt and fat to fruit and veg when cooking, and if you’re buying pre-prepared vegetables, go for ones that don’t have butter or oil added and check the label for salt.
 Starchy carbohydrates - brown varieties are best
Starchy carbohydrates - brown varieties are best
Our diets should also be based around starchy carbohydrates like bread, rice, pasta and potatoes, which provide us with energy.
Choose higher fibre varieties (e.g. wholemeal/brown bread, brown pasta and brown rice) as these get digested more slowly compared to white varieties, which helps us to feel full for longer. We should all aim to eat more fibre to keep our guts healthy and avoid constipation. Adults should eat 30g fibre per day – but we are falling well short of that at the moment. Some brands now offer high-fibre white versions of bread and pasta, so look out for these when you shop. Remember also to avoid adding salt when you cook them.
Less meat and more beans, pulses, fish, eggs and other protein
Along with protein, these foods also provide us with other essential vitamins and minerals like iron and zinc. We should aim to eat at least two 140g portions of fish per week, including a portion of oily fish (e.g. salmon, mackerel and sardines). It is recommended that we eat no more than 500g of red and processed meat per week (about 70g per day), as eating too much can increase the risk of bowel cancer.
Processed meats (like sausages, bacon, cured meats and reformed meat products) offer no real nutritional benefit, and can be high in fat and salt. It’s better to go for high quality fresh, unprocessed meats. Some cuts of meat can be high in fat, particularly saturated fat, so choose leaner cuts with less visible fat, leaner mince and remove the skin from poultry.
Beans and pulses (e.g. lentils, chickpeas) are good alternatives to meat because they are lower in fat and higher in fibre. If you’re buying canned varieties, opt for ones in water with no added sugar or salt.

Dairy and alternatives - watch the fat and sugar
Dairy foods are an important part of the diet, providing protein, vitamins and calcium, which is crucial for healthy bones. Some dairy foods and dairy alternatives can be high in fat and/or sugar (e.g. full fat milk, cheese and flavoured yogurts) but there are healthier options available, including reduced fat cheeses, 1% and skimmed milks, plain low fat yogurts and unsweetened dairy alternatives (e.g. soya milk).
Drinks - choose sugar free varieties
Not only is the food that we eat important, but also what we drink. Sugary drinks are a major source of calories and free sugars in the diet – with some fizzy drinks found to contain as much as 12 teaspoons of sugar per serving! Choose healthier, sugar-free alternatives instead like water, low fat milk, and tea and coffee with no added sugar. Beware of flavoured hot drinks like coffees and hot chocolates with syrups - these can contain more sugar per serving than the entire maximum daily recommended amount for adults.
Putting it all into practice
It’s all well and good knowing what we should be eating, but what we actually choose to eat can be very different. Sometimes the possibility of eating healthily may seem impossible. However, there are some simple tools available to help you make healthier decisions when choosing food on-the-go or doing the weekly shop.
Many coffee shops, sandwich bars and some restaurants now display nutrition information for their products on the shelf or on the menu, so you can see how products and meals compare and go for the healthiest.
Remember to watch portion sizes - when eating out with family and friends why not share a cake, starter or dessert rather than having one each?
Similarly, check the serve size on packaged food and drinks - what is quoted as a serve size on pack may be smaller than what you actually eat or drink, so try and stick to what is recommended.
Use the Foodswitch UK app
With so much choice on the supermarket shelves, and many brands to choose from, deciding which product to buy can be far from easy.
When it comes to nutrition, you might think that all brands are the same, but there can be huge differences in the nutrient content of similar foods and drinks. For example, one brand of flavoured noodles can contain 14 times more salt per serving compared to another! That’s why it pays to check the label and shop around, and using apps like FoodSwitch UK make it easier to find those healthier choices and reduce the amount of fat, sugar and salt in you and your family’s diet.
FoodSwitch UK is a free, independent and simple-to-use smartphone app developed by researchers that helps you find out what is in the food you’re eating so that you can make simple switches to healthier options. It allows users to scan the barcode of a food or drink product and instantly see whether it is high (red), medium (amber) or low (green) in fat, saturates, sugars and salt. The app brings up a list of similar but healthier alternatives to switch to.
The app includes a SaltSwitch filter to help those with, or being treated for, high blood pressure, which displays healthier products with less salt than the product that has been scanned. Users can save healthy favourites on a shopping list ready for next time they shop, and share the information with other users via social media.



Content supplied by Consensus Action on Salt & Health. For more information please visit www.actiononsalt.org.uk/foodswitch
An Update on Trauma and Orthopaedics - Mr John F Nolan MBBS FRCS FRCS(Orth)
We all like to get value for our money.
Over the last 15 years, Trauma and Orthopaedics has led the development of outcome databases in medicine and these now encompass almost all joint replacement surgeries and hip fractures, as well as non-arthroplasty surgery, including ligament reconstruction.
Although originally developed to offer outcome data on implants, the evolution of these increasingly mature and substantial databases is having a significant effect on the way that we, as orthopaedic surgeons practise, with most individuals and departments becoming increasingly aware of the visibility and transparency of the outcomes of their surgical endeavors amongst their peers, their national associations and more widely on NHS websites.
There can be no doubt that all of this has been good for patients and over the last 10 years, the National Joint Registry has clearly demonstrated a 50% reduction in mortality, following hip replacement surgery.
As more than 105,000 hip and nearly 113,000 knee replacements were undertaken in 2018, implant longevity is important and again the best implants, put in well, are performing better than ever.
The National Joint Registry (NJR), which includes data on over 2.5 million joint replacements has recently been taking a close look at the excessive variability of cost of the same prostheses to different hospitals, even within the National Health Service.
The project offers the potential to rationalise and lower the costs of implants to the NHS, leading to more cost effective care.
Patient Reported Outcome Measures (PROMS) and Patient Reported Experience Measures (PREMS) have provided us with details of our patients’ perspective of their “journey” and their quality of life improvements, whilst studies specifically analysing Quality Adjusted Life Years (QALYS) after joint replacement, have confirmed the extraordinary value of this surgery in health economic terms.
NICE has set the threshold for a QALY at around £30,000, with a QALY of less than £10,000 for most hip replacements and in many cases amounting to as little as £1500.
Innovation and prosthesis development remain important for the future and the “Beyond Compliance” initiative from the British Orthopaedic Association (BOA) offers implant manufacturers the opportunity to go over and above the simple requirements of CE marking, facilitating an almost forensic analysis of early results and offering timely identification of any problems. Given the somewhat chequered history of some new implants, the potential benefits to patients are clear.
In the longer term, manufacturers can apply to the Orthopaedic Data Evaluation Panel (ODEP), setup at the request of The National Institute of Health and Care Excellence (NICE), for the award of an implant rating, based on multiple outcome studies. The level of rating awarded is dependent on the quality of evidence available for any prosthesis and includes an assessment of the numbers of implants being considered and the duration of follow-up. After 10 or more years, prostheses are eligible for the coveted 10A* rating, indicating a minimum cohort of 500 hips/knees at the start of the study (consisting of data from beyond the developing centre and from more than 3 centres/surgeons) with a minimum of ten years follow up and an actual revision rate of less than 5%. All deaths, loss to follow up, failures and indications for revisions recorded. A maximum of 20% loss to follow-up is permitted.
As expected, large volume data has facilitated reflective practice leading to the wider adoption of demonstrably more successful techniques, with the use of those implants with better track records now being adopted more widely by the orthopaedic community. The parallel development of more consistent and successful anaesthesia, has contributed to enhanced patient recovery after major surgery and significantly shorter hospital stays.
One-shot spinal anaesthesia associated with either sedation or a light general anaesthetic and local infiltration of longer-acting local anaesthetic agents during the procedure has facilitated early mobilization of patients. Most can walk, fully weight-bearing just 2 or 3 hours after surgery, leading to a reduction in the incidence of thrombotic events, rapid subsequent progress through the patient pathway and safe discharge home from hospital, often after as little as 2 or 3 days.
As local anaesthetics continue to develop, the prospect of significant numbers of hip and maybe even knee replacement patients being treated as day cases becomes a genuine proposition.
In the upper limb, regional an aesthesia, for example brachial plexus blocks, have already transformed the pathway for many patients, with far fewer requiring overnight stays in hospital.
Whilst these trends are set to continue, they depend heavily on established and reliable support services, particularly physiotherapy, being readily available within the communities into which the patients are to be discharged.
“Getting It Right First Time” (GIRFT) started in orthopaedics and represents another exemplar initiative, coming from the British Orthopaedic Association. By collecting a range of outcome data from all the acute hospitals in the country that provide orthopaedic services, a number of outcome parameters have been analysed, (including infection rates), thereby helping to address unwarranted variations between hospitals.
Further, evidence for the concentration of complex procedures in specialist centres is leading to the establishment of hub and spoke networks and whilst some patients are required to travel to regional units, the outcomes of their surgical interventions are improved and costs are reduced.
Increasingly, service funding will need to take account of the concentration of complex cases at specialist units; historically these have been relatively poorly remunerated by tariff, to make this model sustainable.
Perhaps not surprisingly, in these austere times, The Department of Health has shown a great interest in the GIRFT initiative, with methodology being translated to provide similar analyses within other surgical (and medical) disciplines.
Whilst major orthopaedic surgery in grossly obese patients can present real challenges to the surgical, anaesthetic and nursing teams, there is considerable evidence that overweight or moderately obese patients continue to benefit from joint replacement surgery. Their otherwise poor mobility and their pain may lead them to comfort eat and significant weight reduction is often at best difficult and in practice, unobtainable.
Skeletal trauma continues to challenge with its increasing complexity as our population ages and the number of older patients with multiple co-morbidities (and polypharmia), presenting with skeletal failure of one sort or another escalates. Once again, the established registers have helped determine the best surgical interventions for different groups of (eg. hip fracture) patients.
At the other end of the energy spectrum for trauma, Level 1 Trauma Centres offer comprehensive care to multiply injured patients and are associated with demonstrably lower morbidity and mortality rates, once again a result of the development of specialist regional services.
The future is rosy.
Modern bearing surfaces such as ceramics and highly cross-linked polyethylenes are associated with much better wear characteristics than predecessor materials, as demonstrated both in vitro and more importantly, in vivo and the very real expectation of greater prosthetic longevity, even in younger and more active patients.
Technological advances, including 3D printing techniques offer the ultimate of truly bespoke implants when required and when combined with increasingly biocompatible materials such as trabecular metal, provide solutions for complex reconstructions in the presence of very abnormal anatomy.
All this whilst providing great value for money!
John Nolan
Content provided by
Mr John F Nolan MBBS FRCS FRCS(Orth)
Consultant Trauma and Orthopaedic Surgeon
Norfolk and Norwich University Hospital NHS Foundation Trust
Past President, British Hip Society
Dermatology in the NHS: last 70 years - Sriramulu Tharakaram MD FRCPIreland FRCPLondon
 Dermatology as a speciality has made tremendous strides over the past 70 years of the NHS. Once skin diseases were regarded as chronic and hardly treatable but this has changed with advances in dermatology. Today Dermatology has evolved into so many subspecialities including to name some paediatric dermatology, dermatological surgery and lasers, dermatological oncology, contact dermatitis, photobiology, epidermolysis bullosa pioneered in the UK by late Prof Robin Eedy and succeeded ably by Prof John McGrath and Prof Mellerio and and there maybe one or more dermatologists looking after skin rashes in haemato-oncology settings. Powerful drugs are used to treat cancers once untreatably fatal and these produce skin rashes needing dermatology input. Not to forget the research dermatologists making new strides and bringing the products of their effort from the laboratory benches to the patient’s bedside. Whilst all these advances are going ahead Dermatology is also under attack by new changes in the NHS pushing it out of the hospital into the community leaving the in-patients with rashes in a state of limbo; the bidding system also leaving the speciality open for grabs by market forces whose primary objective is monetary under the guise of providing a more efficient service. Some such services have collapsed leaving patients back to where they started!
Dermatology as a speciality has made tremendous strides over the past 70 years of the NHS. Once skin diseases were regarded as chronic and hardly treatable but this has changed with advances in dermatology. Today Dermatology has evolved into so many subspecialities including to name some paediatric dermatology, dermatological surgery and lasers, dermatological oncology, contact dermatitis, photobiology, epidermolysis bullosa pioneered in the UK by late Prof Robin Eedy and succeeded ably by Prof John McGrath and Prof Mellerio and and there maybe one or more dermatologists looking after skin rashes in haemato-oncology settings. Powerful drugs are used to treat cancers once untreatably fatal and these produce skin rashes needing dermatology input. Not to forget the research dermatologists making new strides and bringing the products of their effort from the laboratory benches to the patient’s bedside. Whilst all these advances are going ahead Dermatology is also under attack by new changes in the NHS pushing it out of the hospital into the community leaving the in-patients with rashes in a state of limbo; the bidding system also leaving the speciality open for grabs by market forces whose primary objective is monetary under the guise of providing a more efficient service. Some such services have collapsed leaving patients back to where they started!
In England the largest Dermatology service is the one coming under the St John’s Dermatology Centre, once an independent hospital but now under Guy’s King’s St Thomas’s NHS Trust. Large services exist in Leeds, Birmingham, Newcastle, Manchester and in Cardiff, Edinburgh, Glasgow, Dundee to mention a few.
Whilst the backbone of Dermatological treatments are topical creams and ointments since 1951 when Dr Sulzberger in the USA discovered hydrocortisone, which evolved into more potent fluorinated steroids, Dermatology on both sides of the Atlantic started using drugs used in cancer in low doses to control skin disease as psoriasis with remarkable benefits. Dr Harvey Baker from the London Hospital was one such pioneer. The same Whitechapel hospital carries out breath taking research in molecular dermatology. There are a whole plethora of drugs in Dermatology: acne treated early can leave the patient with virtually normal skin; immunomodulator creams as tacrolimus and pimecrolimus for eczema reduce the fear of skin damage to steroids; psoriasis covering the whole body can be controlled effectively where light and topical treatments seems less effective with the expanding armamentarium of a new class of drugs: Biologics. Crippling rheumatoid arthritis and psoriatic arthritis may soon become a thing of the past.
Dermatologists once regarded themselves as physicians quickly absorbed the American enthusiasm
for surgery and in particular Moh’s surgery invented by Dr Fredrerick Moh from Wisconsin; the procedure where skin cancers are removed under microscopic control virtually guaranteeing full and just enough removal of a skin cancer in strategic parts of the face as eyelids and nose. Dermatologists specialising in Moh’s surgery are always in great demand. A range of treatments exist for skin cancers depending on the type: a cream as 5 Fluorouracil, Aldara, Photodynamic therapy, surgery, radiotherapy and chemotherapy. More importantly the 2 week rule allows GP’s to refer patients who must be seen within 2 weeks for skin cancers with a potential to spread and the regular MultiDisciplinary skin cancer meeting assuring quality control of such skin cancers across the board. The patient gets all this in the tax payer funded NHS without touching his or her purse or worrying about costs.
The history of dermatology in the NHS was recounted in an article written 10 years ago. Some remarkable changes that have occurred are recounted herein.
Infantile Haemangiomas or vascular birthmarks are more common in the white population occurring in 4-10% of infants. They grow rapidly over the first 3-12 months and then spontaneously involute. Treatment is seldom needed unless it ulcerates or causes functional impairment. Treatments were large doses of steroids with a multitude of side effects. UNTIL in 2008 in France Propranolol given to treat a cardiopulmonary condition in an infant with haemangioma resulted in amazing improvement of the haemangioma (Ref: N Eng J Med June 2008): this is now adopted as a first line treatment.
Biologics
These are innovative new therapies engineered to block certain molecular steps that are crucial in the pathogenesis of disease. They have revolutioned the treatment of psoriasis and are used in various other diseases as eczema, urticaria and vasculitis.
Psoriasis: Research into pathogenesis of psoriasis has identified mechanisms of blocking the likely causative pathways. These drugs are referred to as Biologics and include Adalumimab, Etanercept, Infliximab, Ustekinumab, Secukinumab, Ixekinumab. With such treatments it is possible to achieve disease free “clear skin” something which was impossible before. Sometimes these treatments do not work and all such data is pooled by the British Association of Dermatologists Biologics Interventions Register (BADBIR). These are expensive drugs and have to be approved by NICE and there is a vetting process in prescribing them. As patents on these drugs expire drug companies are making slightly cheaper copies or Biosimilars with a modest 10% cost reduction.
Eczema: A proportion of eczema patients do not respond to creams and ointments: these patients are treated with systemic treatments as methotrexate. Sometimes even these do not work. But there is new hope with a biologic Dupilumumab.
Urticaria: Chronic Urticaria or “hives” can sometimes make the affected patients ill and unresponsive to antihistamine and systemic treatments .IgG atoantibodies against IgE were first identified in St John’s Dermatology Centre. A biologic Omaluzimab given subcutaneously to such patients gives them great relief.
Likewise there is hope for autoimmune blistering disorders with Rituximab when all else fails. Lately Alopecia areata (bald patches to total hair loss) and Vitiligo, both autoimmune conditions had few effective treatments can hope for the better with a new category of drugs Janus Kinase inhibitors Tofacitinib, Baricitinib and Ruxolitinib. Vitiligo in the Indian subcontinent is stigmatized as Leprosy adding to the patient’s woes: this treatment not yet available universally may hopefully help immensely.
Melanoma: Melanoma is the most fatal common skin cancer, the fifth most common and the fastest rising cancer in the UK. Whilst excision remains the gold standard some melanomas spread to internal organs. Knowledge of Oncogenes and BRAF has resulted in drugs that inhibit BRAF: vemurafenib/Dabrafenib. Looking at immunogenicity and melanoma newer drugs as Ipilimumab and Nivolumimab also referred to as check point inhibitors help to clear metastases when given which is a stunningly remarkable advance.
Nurses and GP’s in Dermatology Nurses have always played an important role in the development of this speciality. Given the shortage of dermatology consultants nurses have stepped as nurse specialists and nurse consultants working alongside consultants and helping to ease the pressures by contributing a much needed and valued role. GP’s have developed a special interest in dermatology and where well trained are of great help.
Secretaries
With the immense administration needs in the NHS secretaries who do so much are often taken little note of. In DGH settings they often function like a specialist registrar and if you have a good secretary then value them greatly and you will get rich dividends.
Whither Dermatology?
Dermatology like all things is undergoing phenomenal changes; whilst there are great advances happening scientifically these have to be delivered with costs in mind. Perhaps a more integrated and shared service with dermatologists working in hospitals and communities and a nice exchange between teaching and district hospitals enhancing standards overall might help. Whatever advances maybe achieved the patient should be the central focus and the NHS certainly can take pride in quality care delivered free to all those who need.
Acknowledgements: Dr Sophie Momen
Content provided by Srirarmulu Tharakaram, MD FRCPIreland, FRCPLondon, Consultant Dermatologist, Royal Tunbridge Wells, Kent