CCA calls for urgent change to the flu vaccine programme this winter - The Company Chemists’ Association
 It is crucial that the government tells the public how to get the flu vaccination this winter. Patients, particularly those at risk from Covid, need reassurance from health care providers. They will need to know that they can get the vaccine from a community pharmacy in a Covid secure environment which is easy to access.
It is crucial that the government tells the public how to get the flu vaccination this winter. Patients, particularly those at risk from Covid, need reassurance from health care providers. They will need to know that they can get the vaccine from a community pharmacy in a Covid secure environment which is easy to access.
The Company Chemists’ Association (CCA) is the trade association for large pharmacy operators in England, Scotland and Wales. Our members are: Asda, Boots, LloydsPharmacy, Morrison’s, Rowlands Pharmacy, Superdrug, Tesco and Well. Between them, our members own around 6,000 pharmacies representing almost half of the pharmacies in the United Kingdom.
The CCA represents the interests of its members and brings together their unique skills, knowledge and scale for the benefit of community pharmacy, the NHS, patients and the public. Our vision is that everyone, everywhere, can benefit from world class healthcare and wellbeing services provided by their community pharmacy.
The pandemic has changed the delivery of the flu vaccine programme in 2020/21. These changes could have a long-lasting positive impact on flu vaccine targets. They may also lay the groundwork for other programmes, including Covid vaccinations.
The main challenges to delivering flu vaccinations this winter will be:
1. Getting those who at most risk to come forward to get the vaccine first.
This includes the over 65s and people vulnerable to Covid (those with respiratory and endocrine disorders) to protect them from co-circulating flu. Many people who are otherwise healthy have come forward early to get the vaccine. In some parts of the country there has been a ten-fold increase in demand. During the first four weeks of the flu vaccination service, community pharmacists have vaccinated over 650,000 NHS patients – three times the number vaccinated in the same period last year.
It is positive that the benefit of vaccination appears to be landing well with the public this year. However, we also need people to be aware of the process of staging the vaccine to priority groups.
Wholesalers deliver the vaccine to healthcare providers in batches throughout the flu season. Non-priority groups will therefore receive their vaccine in November and December.

2. Reaching targets for priority groups
This year NHS England has set a target of 75% of each priority group to receive the vaccine. Last year the target met was 60%, with variability among cohorts. There are groups that may need specific targeting (e.g. pregnant women). As eligible groups have expanded, reaching these increased targets will be more challenging. As such, it is important that healthcare providers work together to reach patients.
3. Reassurance for nervous patients
We need those in at risk groups to come forward for the vaccine. The necessary safety measures, infection control, distancing and PPE are in place to protect the public in pharmacies. Additional measures such as sending patients information about what to expect from the flu service in advance will help. The vaccination process will be quicker for patients due to the flexibilities introduced this year. These include the removal of the need for written consent and permission for pharmacy to have closed door flu clinics.
We would like to see the following two steps taken to help overcome these challenges:
- Clear and targeted communication to the public, about how this year’s flu vaccine programme is being delivered. This would help reassure those who are eligible for the free NHS vaccine about when and where they can receive it.
- Proposed flexibilities to be come into place for this flu season. The Department of Health and Social Care has proposed widening the Patient Group Direction (PGD) to allow pharmacy technicians to deliver vaccines. We also expect regulations to be laid to allow community pharmacy to deliver in off-site locations including faith centres and community halls.
We believe that these changes, if introduced, could greatly support the future delivery of a Covid vaccine safely and at scale and pace.

Content provided by The Company Chemists’ Association. For more information please visit www.thecca.org.uk
Obesity: Treat and Prevent - An evidence based action plan to reduce death from Covid-19 - Graham MacGregor, Chair of Action on Sugar and Action on Salt Professor of Cardiovascular Medicine
Obesity is a major risk factor for mortality from Covid-19.
These ten recommendations will support the nation to reach and maintain a healthy weight, without placing responsibility solely on the individual and by changing the food environment.
TREAT
Provide guidance for identifying modifiable risk factors
To improve understanding of the many causes of obesity
Increase access and funding for bariatric surgery
Increase access and funding for evidence-based weight loss support
PREVENT
5. Ensure only healthy products are advertised and promoted
6. Adopt fiscal measures to promote healthy food (with income ringfenced to subsidise treatments)
7. Make nutrition labelling mandatory
8. Ensure only healthy food is provided to key workers in their workplaces
9. Improve nutritional profile by incremental reformulation of processed food and drink
10. Set up a new, independent and transparent food watchdog
Obesity and Covid-19
Increasing evidence demonstrates that obesity is an independent risk factor for more severe illness and death from COVID-191,2,3,4,5,6,7,8,9. Data shows that 78% of those infected and 62% of hospital deaths caused by the virus are in overweight or obese individuals1,2. Linking UK COVID-19 data to that of a population cohort (428,225 participants, 340 confirmed COVID-19 hospital cases) and to electronic health records (17,425,445 participants, 5,683 COVID-19 deaths) demonstrates that the more severe the obesity, the more likely to be hospitalised for COVID-19 and/or die from it1,2.
Other risk factors include age, ethnicity, deprivation, and underlying conditions such as heart or kidney disease and type 1 and type 2 diabetes. Obesity is the major risk factor that can potentially be modified meaning millions of people are living with an increased, but preventable, risk from COVID-19.
Treating and preventing obesity
The current NHS10 treatments recommended for severe obesity are bariatric surgery, supported weight loss services, advice, and orlistat, which can be prescribed by a GP. Not all treatments are available or accessible.
Beyond this, although there is an element of personal responsibility in both the treatment and prevention of obesity, this can only be equitably achieved with access to healthy, affordable food in an environment that supports the individual at every turn – not the current obesogenic environment within which we live11. Long planned and vital governmental measures to address this have been delayed by food industry lobbying and have now been put on hold due to the COVID-19 outbreak, at a time when they have never been more necessary.
The Childhood Obesity Plans chapters 2 and 3 (Prevention Green paper) and the Independent Report by the outgoing Chief Medical Officer make a series of recommendations to improve the nation’s health, focusing on children, but with evidence that they will contribute to preventing adult obesity via their impact assessments (Appendix 1). So far only the Sugar Reduction Programme and the Soft Drinks Industry Levy have been implemented. The status of the remaining recommendations, which Public Health England have repeatedly stated are needed, and how they are connected to the ten actions, are outlined in Appendix 1.
Action on Sugar and Action on Salt’s evidence-based action plan for the Prime Minister and government departments builds on accepted evidence and recommends stricter parameters necessary for the urgent nature of the pandemic. We ask for the government to immediately implement all these measures to help protect and support those living with obesity during the pandemic, whilst also improving health for all in the long term.
TREAT
Immediately put support in place for individuals to reach and maintain a healthy weight
1. Provide guidance for identifying modifiable risk factors
We recommend that the government provides guidance for self-identification of modifiable risk factors, in particular, weight status. Current recognised measures include Body Mass Index (BMI), waist circumference and the waist-hip ratio. For most people, BMI is a relatively straightforward, accurate and convenient way of assessing your risk12. Covid-19 data has shown that as the reported BMI increases, the risk of having severe illness from Covid-19 increases13. At this time it is not possible to access GP surgeries and other means of identifying risk, so it is vital that information is provided to encourage people to make these calculations at home to identify their risk.
2. To improve understanding of the many causes of obesity
Obesity is not a choice. Blame should not be placed on the individual, but instead there must be more emphasis on creating an environment that supports people living with obesity and prevents rather than encourages people to become obese. The existing and recognised framework to communicate the multifactorial root causes of obesity should be immediately implemented across government, NHS, the food industry, technology companies and the media14. This framework is designed to support those working in the field of obesity to communicate and work in a non-stigmatising manner relating to body weight or size, and to take the emphasis off personal responsibility.
3. Increase access and funding for bariatric surgery
Bariatric surgery or metabolic surgery is effective at treating those individuals with extreme obesity (BMI>40+). Patients can only be considered if they can demonstrate that they have tried various lifestyle changes which are often impossible to undertake within our current food environment, putting further distress on the individual. This surgery is a major operation and should not be taken lightly, however it should be properly funded to reduce waiting times to expediate access for high risk individuals. Currently the majority of individuals who would qualify for bariatric surgery are not able to access them due to limited funding for the NHS15.
4. Increase access and funding for evidence-based weight loss support
Fad diets are ineffective in the long term. There are some effective weight management support services for those that are suitable, however, access to these services through the NHS is limited and under-funded, with extensive waiting lists. Evidence based weight management services are available in some areas but are often dependent on stretched local authority funding, and are not accessible to everyone. Multi-disciplinary supported weight loss services should be adequately funded and signposted and their long-term effectiveness needs to be researched further, including the effectiveness of personalised technology16.
PREVENT
The following ‘pandemic response’ measures build upon the existing evidence-based recommendations committed to by this government in the Childhood Obesity Plan Chapters 2 and 3 (Prevention Green Paper) and Time to Solve Childhood Obesity: An Independent Report by the Chief Medical Officer.
5. Ensure only healthy products are advertised and promoted
Advertising, price and placement promotions (such as end of aisles, point of sale) of more unhealthy foods and drinks manipulates choice, creating an environment where products high in salt, sugar and/or fat are more desirable. Food and drink companies should be banned from advertising any food or drink high in fat, salt or sugar (HFSS), as defined by the new Nutrient Profile Model17. There must also be mandatory restriction of price, point of sale and location promotions on all products high in salt, sugar and/or fat in all outlets where food and beverages are sold (including deliveries and online).
6. Adopt fiscal measures to promote healthy food (with income ringfenced to subsidise treatments)
In order to subsidise the expansion of weight management services provided by the NHS (actions 3 & 4), this government needs to raise revenue through ring-fenced fiscal measures.
The Soft Drinks Industry Levy has been successful in reducing sugar intakes via reformulation, and in raising much needed revenue for children’s services. The current sugar levy thresholds should be reduced, the rates increased, and it should be immediately applied to a calorie threshold in sugar sweetened milk and milkalternative drinks.
The current voluntary reformulation programmes have failed. Incremental mandatory reformulation targets must be set for salt, sugar and calories. Policed by a new independent food watchdog.
Fiscal measures that could be explored to enforce this could include:
- Reformulation Levy: for non-compliance with the reformulation targets within the sugar and salt reduction programmes and the overdue calorie reduction programme
- Energy Density Levy: for all calorie dense, nutritionally poor, processed foods
- VAT Reform/subsidies: Using the VAT system to promote healthy food, as defined by the new Nutrient Profile Model (NPM)
- Planning restrictions: Make it more difficult to open unhealthy food outlets and encourage healthier outlets by using a ‘nutrition rating scheme’ monitored by a new food watchdog18.
7. Make nutrition labelling mandatory
This government needs to seize on the opportunity of Britain’s exit from the EU and make colour-coded signpost labelling mandatory on all food, drinks and alcohol sold in retail, and to introduce calorie labelling for the out-of-home sector. While the out of home sector has been impacted by the virus, large, multinational food companies have been able to reopen, largely in more deprived areas and with limited menus which predominately feature HFSS products. Starting with companies with the resources to open, customers should be provided with nutrition information at the point of sale. Support and expertise should be provided by a new food watchdog.
8. Ensure only healthy food is provided to key workers in their workplaces is healthy
Key workers should have access to the highest nutritional quality food at their workplaces. This government must ensure all food provision to all key workers and others in public sector meets nutrition and sustainability standards, as set out in the Government Buying Standards. This includes schools, hospitals etc.
9. Improve nutritional profile of processed food and drink
This government must push forward with proposals to make long term and meaningful improvements to nutritional profile of processed food and drink. Nutritional quality can be improved by reducing excessive calories through sugar, saturated fat and/or alcohol content reduction, reducing salt, and increasing fruit, vegetable, fibre and micronutrients. This government can implement portion size restrictions for the food industry including the hospitality sector to adhere to, based on energy density, and ensure that all new products meet set thresholds for sugar, salt, calories and limits on the level of processing19.
10. Set up a new, independent and transparent food watchdog
A new, independent and transparent food watchdog, free from ministerial, industry and other vested-interest influences, should be immediately set up. This will enable them to make clear, independent, evidence-based information widely and freely available whilst working with technology companies and media outlets to halt
the spread of misinformation.
This new watchdog must put the primary focus on healthy diets, with physical activity encouraged for general health improvement. The watchdog should be well funded, for research and agility to respond to new evidence and innovative solutions.
For these treatment interventions to be effective the above measures for preventing obesity need to be actioned immediately.
“The UK is facing two major pandemics. One immediately, Covid-19 and the other a longer-term crisis with obesity. Clear evidence has emerged that the two pandemics interact. This is a major opportunity for the government and the food industry to prevent unnecessary suffering and death.”
Graham MacGregor
Chair of Action on Sugar and Action on Salt
Professor of Cardiovascular Medicine
Action on Sugar
Action on Sugar is a group of scientific experts concerned with sugar and obesity and its effects on health. It is working to reach a consensus with the food industry and Government over the harmful effects of a high calorie diet, and bring about a reduction in the amount of sugar and fat in processed foods to prevent obesity and type 2 diabetes.
@actiononsugar
actiononsugar.org
Action on Salt
Action on Salt is a group concerned with salt and its effects on health, supported by 25 expert scientific members. Action on Salt is successfully working to reach a consensus with the food industry and Government over the harmful effects of a high salt diet, and bring about a reduction in the amount of salt in processed foods as well as salt added to cooking, and the table, to prevent high blood pressure and cardiovascular disease.
@actiononsalt
actiononsalt.org.uk
References
Throughout the article, ‘sugar’ refers to ‘free sugars’ and ‘drink’ refers to both alcoholic and non-alcoholic drinks.
--------------------------------
1 Ho FK, Celis-Morales CA, Gray SR, et al. Modifiable and non-modifiable risk factors for COVID-19: results from UK Biobank. medRxiv 2020. [Epub ahead of print]
2 The OpenSAFELY Collaborative, Williamson E, Walker AJ, et al. OpenSAFELY: factors associated with COVID-19-
related hospital death in the linked electronic health records of 17 million adult NHS patients. medRxiv 2020. [Epub ahead of print]
3 Simonnet A, Chetboun M, Poissy J, et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity (Silver Spring, Md) 2020. [Epub ahead of print]
4 Lighter J, Phillips M, Hochman S, et al. Obesity in patients younger than 60 years is a risk factor for Covid-19 hospital admission. Clin Infect Dis 2020. [Epub ahead of print]
5 Yu T, Cai S, Zheng Z, et al. Association Between Clinical Manifestations and Prognosis in Patients with COVID-19. Clin Ther 2020. [Epub ahead of print]
6 Kalligeros M, Shehadeh F, Mylona EK, et al. Association of Obesity with Disease Severity among Patients with COVID-19. Obesity (Silver Spring, Md) 2020. [Epub ahead of print]
7 Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospitalization and critical illness among 4,103 patients with COVID-19 disease in New York City. medRxiv 2020. [Epub ahead of print]
8 Ong SWX, Young BE, Leo YS, Lye DC. Association of higher body mass index (BMI) with severe coronavirus disease 2019 (COVID-19) in younger patients. Clin Infect Dis 2020. [Epub ahead of print]
9 Huang R, Zhu L, Xue L, et al. Clinical findings of patients with coronavirus disease 2019 in Jiangsu province, China: A retrospective, multi-center study. PLoS Negl Trop Dis 2020; 14: e0008280.
10 NHS. Treatment of Obesity: https://www.nhs.uk/conditions/obesity/treatment/
11 HHSC. Time to solve childhood obesity: CMO special report: https://www.gov.uk/government/publications/time-tosolve-childhood-obesity-cmo-special-report
12 NHS. Healthy Weight Calculator: https://www.nhs.uk/live-well/healthy-weight/bmi-calculator/
13 Green WD, Beck MA. Obesity Impairs the Adaptive Immune Response to Influenza Virus. Ann Am Thorac Soc 2017; 14: S406-S9.
14 Dr Stuart W., Scaled Insights and Obesity UK. Positive Communication About Obesity: https://static1.squarespace.com/static/5975e650be6594496c79e2fb/t/5e5c1158bd974c78734258de/1583092058005/Positive+Communication+About+Obesity.pdf
15 Rubino F et al. Bariatric and metabolic surgery during and after the COVID-19 pandemic: DSS recommendations for management of surgical candidates and postoperative patients and prioritisation of access to surgery.Lancet, 2020, S2213-8587(20)30157-1
16 NHS England. Prevention Tier 2 weight Management Services: https://www.england.nhs.uk/ltphimenu/prevention/tier-2-weight-management-services/
17 Department of Health. 2011. The Nutrient Profiling Model https://www.gov.uk/government/publications/the-nutrientprofiling-model: (New Nutrient Profile Model (NPM) to be immediately released and replace current NPM and measures of food and drinks High in Salt, Fat and Sugar (HFSS))
18 The Food Standards Agency Food Hygiene Rating Scheme: https://www.food.gov.uk/safety-hygiene/food-hygienerating-scheme
19 NOVA classification system: http://www.fao.org/3/ca5644en/ca5644en.pdf
Content provided by Graham MacGregor, Chair of Action on Sugar and Action on Salt, Professor of Cardiovascular Medicine.Content provided by Graham MacGregor, Chair of Action on Sugar and Action on Salt, Professor of Cardiovascular Medicine. For more information please visit actiononsugar.org and actiononsalt.org.uk.
Portable hand-held self-monitoring blood cholesterol devices for the monitoring of patients on lipid lowering treatment - J Bolodeoku MBBS, MSc, MBA, DPhil, FRCPath
Point of Care Testing (POCT) in the monitoring of hypertensive and diabetic patients for blood pressure and glucose has been shown to be beneficial 1,2,3,4,5,6,7,8.
In the management of patients with hyperlipidaemia, it is the normal practice that after initiating pharmacological interventions such as statins, fibrates, bile acid sequestrants and more recently, PCSK9 inhibitors, the patients are expected to have follow up laboratory test done at some appropriate time point. Patients will usually have these blood tests done at the local hospital laboratory or General Practice (GP) who would have the blood sample sent to the local hospital laboratory prior to their visit in order to have the cholesterol estimations ready for their out-patient visit. This way of conducting blood cholesterol measurements is not optimum as most clinicians are usually making a judgement call on one blood lipid profile estimation when the more optimum procedure will be to make the call after a review of more than one lipid profile. This would require the patients to attend the local hospital laboratory or General Practice (GP) at least more than once (route A in figure 1), this could be quite a bother to patients and therefore the question is can portable hand-held self-monitoring of blood cholesterol (SMBC) (route B in figure 1) be of benefit in the management of these patients?
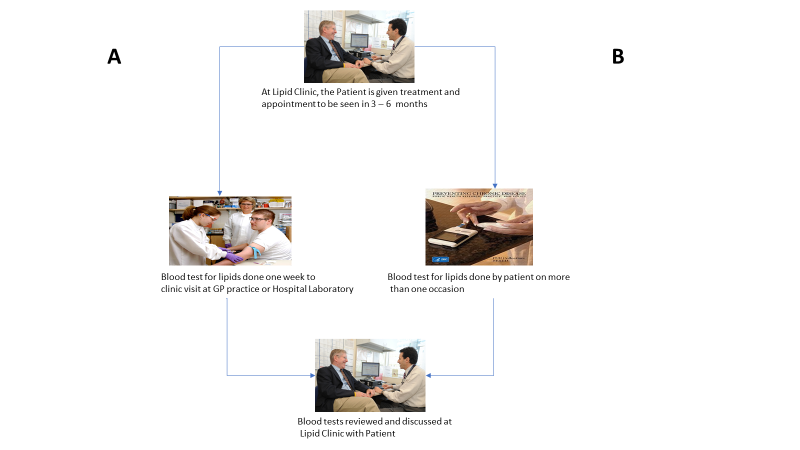
Figure 1 - Showing routes A and B in the monitoring of blood cholesterol in a lipid clinic
The POCT devices for measuring cholesterol vary from hand-held self-monitoring blood cholesterol devices such as the Accutrend Plus, BeneCheck Plus, CardioChek PA, Cholestech LDX®, Veri-Q, 3in1, the elemark™, to the compact desktop analyser such as the Cholestech LDX®. They measure a number of lipid fractions (total cholesterol, triglycerides, high density lipoprotein, low density lipoprotein) and ratios on whole blood, plasma or serum collected from the finger or venous blood using reflectance or biosensor technology with single-use, disposable, dry reagent test strips, rotors or cassettes. The Cholestech LDX is one of the well-studied lipid testing POCT devices but it is a desk top analyser, this review focuses on the portable handheld self-testing devices such as the Accutrend Plus, BeneCheck Plus, CardioChek PA, Veri-Q, 3in1 and the elemark™.
There are several factors that should be considered that will influence the lipid estimations such as the accuracy, the precision and practical usage of the devices and the person day to day lipids variation. These factors will be discussed in relation to several of the portable hand-held self-monitoring blood cholesterol devices on the market and in the literature.
Accuracy
The CardioChek PA was one of the two point-of-care (POC) cholesterol testing devices that was directly compared to a laboratory method using a venous sample to determine device accuracy. The conclusion was that the device produced clinically equivalent values when compared to the same patients’ samples analysed in a reference laboratory and operated within industry accuracy standards11,12. The Accutrend® Plus total cholesterol (TC) and triglyceride (TG) concentrations correlated very well (r >0.80) with laboratory reference method used13. Recently, TC, and TG results from the elemark™ device were shown to correlate very highly with those of laboratory method using the AU5800 Analyzer (Beckman Coulter Inc., IN, USA)14.
Precision
The laboratory analytical precision is measured as coefficient of variation percent (CV%). The Cholesterol Reference Method Laboratory (CRMLN) cholesterol certification criteria for total cholesterol (TC) is < or = 3%, for and high density lipoprotein-cholesterol (HDL-C) is < or = 4% and for low density lipoprotein-cholesterol (LDL-C) < or = 4% and HDL-C < or = 4% and the National Cholesterol Education Programme (NCEP) recommended precision performance criteria for laboratory TC is < or = 3% and HDL-C < or = 6%15,16. The precision (within and within-run precision) for the CardioCheK PA, was 3.7% for total cholesterol and 6.2% for HDL-C for level 1 concentration and 3.6% for TC and 3.5% for HDL-C for level 2 concentration17. In an evaluation by the UK NHS Purchasing and Supply Agency of the CardioChek PA, showed for TC an imprecision of 12%, for HDL-cholesterol 22% and for TG 14%10. In a recent study, it was shown that there was comparable precision between the FDA cleared, CE marked, CLIA waived and CRMLN certified CardioChek PA and the elemark™. The lipid precision profile of both devices (CardioChek PA - 5.4 – 8.3% for TC, 3.4% – 5.5% for HDL-C, 9.4% – 14.0% for LDL-C and elemark™ - 3.0% – 5.3% for TC, 4.3% – 6.2% for HDL-C and 5.5% – 14.4% for LDL-cholesterol)18. In addition, the inter-assay precision of the Multicare Cholesterol system was 4.51% (range, 2.38% - 8.54%) for TC and 3.29% (range, 1.06% - 7.45%) for TG19.
Biological Variation
Lipid concentrations vary within the course of the day and the ranges of within person biological variability (expressed as the coefficient of variation percent) that have been described in the literature for healthy volunteers, shows the CV% ranges for total cholesterol is 2.5% - 10.9%, for HDL-cholesterol is 3.6% - 12.4%, for LDL-cholesterol 7.8% - 13.6% and for triglyceride 12.9% - 40.8%20-23. The within person day to day variation in a healthy volunteer was assessed using three of the cholesterol testing POCT devices, the 3in1, CardioChek PA and elemark™ and their respective CV% fell within the CV% described in the literature: for the 3in1, total cholesterol 6.9% and triglyceride 34%; for the CardioChek PA, total cholesterol 9.4%, triglyceride 23% HDL-cholesterol 7.0%, LDL-cholesterol 14% and triglyceride 23.11%; for the elemark™ total cholesterol 5.0%, triglyceride 30% HDL-cholesterol 13% and LDL-cholesterol 13%24.
Practical Usage
The MultiCare system was easy to be used by patients, when their self measured estimations of either total cholesterol or triglyceride were compared with the results of a professional operator performed on the same device. On a second sample, there was very good correlation (r= 0.978) with a mean difference of 0.28% between the two sets of results19. In a randomised study, investigating the value of home monitoring of lipids, one group of patients received the hand-held device (CardioChek PA) and measured and reported their lipid levels for 6 months using a phone call, whilst the other group had their lipids measured in the usual care group in a traditional laboratory setting. The results showed that mean LDL-C decreased from 186 mg/dL (4.8 mmol/L) to 117 mg/dL (3.0 mmol/L). In the usual care group, whilst a similar reduction of LDL-C decrease from 162 mg/dL (4.2 mmol/L) to 105 mg/dL (2.
7 mmol/L) was observed in the patients using the home monitoring, there was no significant difference between the mean changes. In addition, there was also no significant difference between the two groups with regards to mean changes in HDL-C and triglycerides25. Recently, we evaluated the performance (intra-individual variation, intra-assay precision and comparative data) of the 1drop™ smart phone in measuring total cholesterol. 1drop™ Smartphone is a smart phone (figure 2) used to determine total cholesterol. In this pilot study, on a healthy volunteer, the 1drop™ demonstrated a within in person variation CV% of total cholesterol of 7.3% and an intra-assay precision of 6%. In the comparative study, the total cholesterol estimates of the 1drop™ device were on average 6%, 13% and 23% more than the total cholesterol estimates of the Mission, Prima 3in1 and CardioChek, respectively27.

Figure 2 - Figure showing photograph Galaxy J3 with the specially designed smartphone cover and membrane containing dried reagents (1drop™ TC total cholesterol test cartridge)
In conclusion, the portable hand-held self-monitoring blood cholesterol devices correlate very well with the traditional laboratory cholesterol methods. Even though it appears that both the precision criteria (CRMLN and NCEP) are quite stringent for the portable hand-held self-monitoring blood cholesterol devices, as all of the devices exceeded the expected analytical precision for TC of < or = 3%, for HDL-C of < or = 4%/6% and for LDL-C of LDL-C < or = 4%, they have a reasonable precision profile and they can be used very well by patients. This review highlights the potential of self monitoring hand-held devices to be used in the management of patients undergoing therapeutic intervention, where there is a requirement to monitor the lipid levels in response to the interventions. There is a need for more real-world experience in the use of these devices, in the management of these patients, in the primary and outpatient settings, to fully understand the true benefit and impact these devices have in the management of patients undergoing therapeutic intervention. Hopefully as self-monitoring of blood glucose is routine in the management of patients with diabetes mellitus, self-monitoring of blood lipids will become routine in the management of patients undergoing treatment and monitoring of their lipid profiles.
References
- Crook MA. Near patient testing and pathology in the new millennium. Journal of Clinical Pathology 2000; 53: 27 – 30
- Kilgore ML, Steindel SJ, Smith JA. Evaluating stat testing options in an academic health centre: therapeutic turnaround time and staff satisfaction. Clin Chem 1998; 44 (8) : 1597 – 1603
- Rainey PM. Outcomes assessment for point-of-care testing. Clin Chem 1998; 44 (8) : 1595 – 1596
- Price CP. Regular review: Point of care testing. BMJ 2001; 322 : 1285 – 1288
- Hobbs R. Near patient testing in primary care. BMJ 1996; 312 : 263 – 264
- Price CP. Delivering clinical outcomes. Point-of-Care-Journal of Near Patient Testing and Technology 2003; 2 (3) : 151 – 157
- Cottrell E, Chambers R, O’Connell P. Using simple telehealth in primary care to reduce blood pressure; a service evaluation. BMJ Open 2012;2:e001391
- Klonoff DC. Benefits and Limitations of self-monitoring of blood glucose. J Diabetes Sci Technol 2007; 1 : 130 – 132
- Pluddermann A, Thompson M, Price CP, Wolstenholme J, Heneghan C. Point of care testing for the analysis of lipid panels. Br J Gen Pract 2011; DOI: 10.3399/bjgp12X630241
- Centre for Evidence Based Purchasing. CEO catalogue search. London. Department of Health http://www.healthcheck.nhs.uk/document.php?o=11 (accessed 3 Aug 2017)
- Dale RA, Jensen LH, Krantz MJ. Comparison of two point of care lipid analyzers for use in global cardiovascular risk assessment. Ann Pharmacother 2008; 42 (5) 633 – 639
- Shephard MD, Mazzachi BC, Shephard AK. Comparative performance of two point of care analyzers for lipid testing, Clin Lab 2007; 53 (9-12): 561 – 566
- Scafoglieri A, Tresignie J, Provyn S, Clarys JP, Bautmans I. Reproducibility, accuracy and accordance of Accutrend® Plus for measuring circulating lipid concentrations in adults. Biochemia Medica 2012; 22 (1) : 100 - 108
- Yun K, Lee J, Choi J, Song I-U, Chung Y-A. Smartphone based point of care lipid blood test performance evaluation compared with a clinical diagnostic laboratory method
- National Cholesterol Education Program Laboratory Standardization Panel. Current status of blood cholesterol measurement in clinical laboratories in the US. Clin Chem 1988; 34: 193-201
- National Cholesterol Education Program Laboratory Standardization Panel. Recommendations for measurement of high density lipoprotein cholesterol; executive summary. Clin Chem 1995; 41 : 1427-1433
- Whitehead SJ, Ford C, Gama Rousseau. A combined laboratory and field evaluation of the Cholestech LDX and CardioChek PA point of care testing lipid and glucose analysers. Ann Clin Biochem 2013; 51 (1) : 54–67
- Bolodeoku J, Pinkney S, Imprecision evaluation of self monitoring of blood cholesterol (SMBC) handheld point of care testing devices: Elemark™ and CardioChek PA. Ann Clin Lab Res Vol. 7 No. 1: 290
- Rapi S, Bazzini C, Tozzetti C, Sbolci V, Modesti PA. Point of care testing of cholesterol and triglycerides for epidemiologic studies: evaluation of the MultiCare in system. Translational Research 2009; 153 (2) : 71–76
- Hammond J, Wentz P, Statland BE, Phillips JC, Winkel P. Daily variation of lipids and hormones in sera of healthy subjects. Clinica Chimica Acta 1976; 73 (2) : 347 – 352
- Demacker PNM, Schade RWB, Jansen RTP, Laar AV. Intra-individual variation of serum cholesterol triglycerides and high density lipoprotein cholesterol in normal humans. Atherosclerosis 1982; 45 (3) : 259 – 266
- Gidding SS, Stone NJ, Bookstein LC, Laskarzewski PM, Stein EA. Month to month variability of lipids, lipoproteins and apolipoproteins and the impact of acute infection in adolescents. The Journal of Pediatrics 1998; 133 (2) : 242 – 246
- Bookstein L, Gidding SS, Donovan M, Smith FA. Day to day variability of serum cholesterol, triglyceride and high density lipoprotein cholesterol levels. Arch Intern Med 1990; 150 (8) : 1653 – 1657
- Bolodeoku J. Biological Variation of Self-Monitoring of Blood Cholesterol (SMBC) Using Portable Handheld Point of Care Testing Devices: 3in1, CardioChek PA and Elemark. Curr Trends Med Diagn Meth 2018: CTMDM-106. DOI: 10.29011/ CTMDM-106.100006
- Alkouli MA, Carry BJ, Jarrett H, Sirna SJ. Management of hypercholesterolaemia utilizing a home lipid monitoring system; preliminary findings. J Clin Lipid 2013; 7 (3) : 254 – 255
- Taylor JR, Lopez LM. Cholesterol point of care testing. Ann Pharmacother 2004; 38 (7-8) : 1252 – 1257
- Bolodeoku J, Clark S, Anyaeche C. Self-monitoring of blood cholesterol (SMBC) using the total cholesterol testing cartridge on the 1drop™ smartphone. Biomed J Sci & Tech Res 29 (2)-2020 BJSTR.MS.ID.004760
Content provided by J Bolodeoku MBBS, MSc,
MBA, DPhil, FRCPath
Address:
Lipid Clinic, Department of Cardiology
Basingstoke & North Hampshire Hospital
Aldermaston Road, Basingstoke
Hampshire, United Kingdom
RG24 9AN
This email address is being protected from spambots. You need JavaScript enabled to view it.
Tel No. +44 07765401135