Refuge has been empowering and supporting women to rebuild their lives for the last 50 years - Refuge
 The economic conditions for survivors to leave their perpetrators are already wholly unfavourable, with finances often acting as a barrier to leaving an abuser. Perpetrators often control household income, which makes it harder for survivors to access the money they need to flee. The cost-of-living crisis has meant that for women experiencing domestic abuse, life and death decisions just got even harder.
The economic conditions for survivors to leave their perpetrators are already wholly unfavourable, with finances often acting as a barrier to leaving an abuser. Perpetrators often control household income, which makes it harder for survivors to access the money they need to flee. The cost-of-living crisis has meant that for women experiencing domestic abuse, life and death decisions just got even harder.
Approximately 73% of our frontline staff surveyed have said that the cost-of-living crisis is increasing barriers to leaving a perpetrator and 68% stated that it was leading to survivors questioning whether they made the right decision to leave their perpetrator due to struggles to afford the basics. Some frontline workers report that women have returned to perpetrators as they cannot afford to live alone or as a single parent.
Now as prices rise, while pay and benefits do not, it just got even harder for women to leave an abusive partner. Many survivors’ benefits have been paid into their partner’s account. Many wait around six weeks to get universal credit when they flee their partner and end up struggling. Imagine the fear of leaving your home to build a new life without a penny in your pocket. Some women will check their balance and feel they simply can’t afford to reach safety.
As the country’s largest provider of specialist domestic abuse services, we know it can take women up to seven attempts to leave an abuser. Desperately trying to get enough money to survive on your own and coming short is enough to scare women back to an abusive partner. Refuge has been empowering and supporting women to rebuild their lives for the last 50 years. Refuge runs emergency accommodation, community services, and the National Domestic Abuse Helpline.
We help make sure women looking for a safe place and support can find it. We make sure women get clothes that make them feel like themselves again. We give toys to children that take their minds off things they should never have seen. We help women take control of their lives again. We give women fleeing an abusive partner a refuge space where they can recover and build a new life. We support survivors to use phones and computers without being found by their abuser.

We provide translators to survivors so they can access the support they need, removing language barriers. We support women who’ve been controlled financially with things like bank accounts and benefits.
We know we can always count on our community to send an unmistakable message: we stand with women experiencing domestic abuse, always. Absolutely no woman should pay for the cost-of-living crisis with her life - and together, we’ll make sure of it. Thank you for standing with us.
Content provided by Refuge. For more information please visit www.refuge.org.uk.
The natural history of COVID-19 means that its prevention is challenging - Professor Hugh Pennington
About 150 years ago we began to leave the period in human history dominated by frequent and repeated pandemics.
Separating human faeces from drinking water and better diets were crucial. We began to live longer. Then in the early twentieth century, thanks to vaccines, infectious disease hospitals and, finally, antibiotics, life expectancy increased even faster. Children were no longer routinely carried off by infection. We moved into an age dominated by degenerative and man-made conditions, typified by coronary artery disease and strokes. But half-century ago, and unexpectedly, as causes of premature deaths their incidence began to decline, creating a population of elderly people who because of their age are as susceptible today to some pathogens as undernourished children in the UK in Dickensian times were to measles and tuberculosis. It was said at the end of the twentieth century, well before COVID-19 emerged, that we now live in the age of the re-emergence of infectious diseases. Prescient indeed. The linear relationship between age and infection mortality is stronger for Covid-19 than for any other pathogen.
So infection control is more important than ever. Prevention must be paramount. It is easy to identify failures. The common use of the caveat that the death in hospital of a person with a COVID-19 positive test may well mean that they were infected after admission but possibly died from the condition that led to their admission, not COVID-19, shows the frequent acceptance of an event that might have been preventable.
To be fair, the natural history of COVID-19 means that its prevention is challenging. Not only does the virus spread on the air, but individuals infected with the virus can spread it before they develop symptoms. Superspreading (overdispersion) is common. Current vaccines are far better at preventing a lethal outcome from an infection than preventing an infection in the upper respiratory tract and concomitant spread of the virus, and vaccine immunity and that generated by an infection wanes quite quickly. The closest parallel is influenza, with its spread by aerosol, its evolution in real time, the limited protection delivered by vaccines, and its historical pandemic record. It is a prime candidate as the cause of the next pandemic.
When I qualified in medicine, I took career advice and was told that infectious disease was a dying specialty because of vaccines and antibiotics. I ignored my advisors and, sad to say, was right to do so. Antibiotic resistance is a much bigger challenge today than when Alexander Fleming predicted it in his Nobel Prize lecture in 1945. There are no vaccines against Staphylococcus aureus. MRSA evolved. It has not gone away. Norovirus and Campylobacter are common. Respiratory syncytial virus is still with us. And new challenges will continue to take us by surprise. Nobody predicted that monkeypox would  recently come out of its natural home in Africa and cause cases world-wide. Controlling infections by it requires bespoke procedures. It is the same for COVID-19, norovirus, Campylobacter, respiratory syncytial virus, MRSA and influenza. As a medical microbiologist I declare an interest. The COVID-19 pandemic has been kicked into touch as an influence on practice, with “learning lessons” being left to public inquiries. They take years, and their track record in that regard is not good. I conducted two inquiries into lethal E.coli O157 outbreaks and concluded the second one with Hegel’s aphorism: “What experience and history teach is this - that people and governments have never learned anything from history or acted upon principles deduced from it”.
recently come out of its natural home in Africa and cause cases world-wide. Controlling infections by it requires bespoke procedures. It is the same for COVID-19, norovirus, Campylobacter, respiratory syncytial virus, MRSA and influenza. As a medical microbiologist I declare an interest. The COVID-19 pandemic has been kicked into touch as an influence on practice, with “learning lessons” being left to public inquiries. They take years, and their track record in that regard is not good. I conducted two inquiries into lethal E.coli O157 outbreaks and concluded the second one with Hegel’s aphorism: “What experience and history teach is this - that people and governments have never learned anything from history or acted upon principles deduced from it”.
The NHS is being “reformed” again. It would be a scandal if the training and support of those involved in infection control isn’t prioritised. Preventing the preventable save lives and frees up time for all parts of the NHS to deal with the unpreventable challenges they face. Not only does it save money, but as Hans Zinsser said in his plague literature classic “Rats, Lice and History”: ”Infectious disease is one of the few genuine adventures left in the world. The dragons are all dead, and the lance grows rusty in the chimney corner. But however secure and well-regulated civilized life may become, bacteria, protozoa, viruses infected fleas, lice, ticks, mosquitoes and bedbugs will always lurk in the shadows ready to pounce. About the only genuine sporting proposition that remains unimpaired… is the war against these ferocious little fellow creatures”.
Thomas Hugh Pennington, CBE, FRCPath, FRCP, FMedSci, FRSE is emeritus professor of bacteriology at the University of Aberdeen, Scotland.
‘COVID-19: The Postgenomic Pandemic’ is the title of his book about COVID-19 science, which was published in August 2022 to critical acclaim.
Technology-enabled Virtual Wards have arrived, are you ready? - Masimo
 The NHS must establish 24,000 Virtual Ward beds by December 2023 to support a targeted increase of 30% in elective care procedures by 2025. Masimo SafetyNet®, a Digital Health platform from Masimo, can help deliver effective technology-enabled “Virtual Ward” outside of the hospital, using reliable, trusted, proven and privacy-compliant solutions for timely detection, prevention, and treatment of patients. Virtual Wards aim to achieve admission avoidance, early discharge, increasing workforce efficiency and enhancing patient experience.
The NHS must establish 24,000 Virtual Ward beds by December 2023 to support a targeted increase of 30% in elective care procedures by 2025. Masimo SafetyNet®, a Digital Health platform from Masimo, can help deliver effective technology-enabled “Virtual Ward” outside of the hospital, using reliable, trusted, proven and privacy-compliant solutions for timely detection, prevention, and treatment of patients. Virtual Wards aim to achieve admission avoidance, early discharge, increasing workforce efficiency and enhancing patient experience.
Masimo SafetyNet®, is more than just an app, its clinical portal offers over 150 customisable live care programs, at no charge, across the full range of patient pathways, both “pre” and “post” hospital stay. Both a command centre and a patient-centric view are provided to support review of the data in a variety of ways. Patients and acute care providers connect via the secure, NHS NDG compliant Masimo SafetyNet network, enabling 2-way audio and video communication on a 24/7 patient specific basis. Masimo SafetyNet can be integrated seamlessly with existing Electronic Health Records, keeping all patient data in one easy to access location.
Wireless wearable sensors, both spot-check and continuous, are seamlessly integrated via Bluetooth with patient’s own mobile devices. Masimo SET® Measure-through Motion and Low Perfusion technology ensures high hospital-grade monitoring standards for all patient populations. Alert limits, designed to automatically notify the acute care providers when the patient shows signs of deterioration, allow providers to target interventions and prioritise patient management as needed.
For Patients: Technology-enabled Virtual Wards help assure higher-acuity patients that they remain under the watchful eye of clinicians even following discharge to their own home.
For Acute Care Providers: Masimo SafetyNet offers advanced automation features so institutions can more easily deploy home monitoring, track patient compliance, identify when intervention may be required, and prioritise patient needs whilst maintaining the ability to scale up to meet patient demand.
For NHS Leaders: Masimo SafetyNet is an effective, easily deployed turnkey solution designed to address the challenge of rapidly establishing and operating Virtual Wards whilst optimising use of clinical resources.
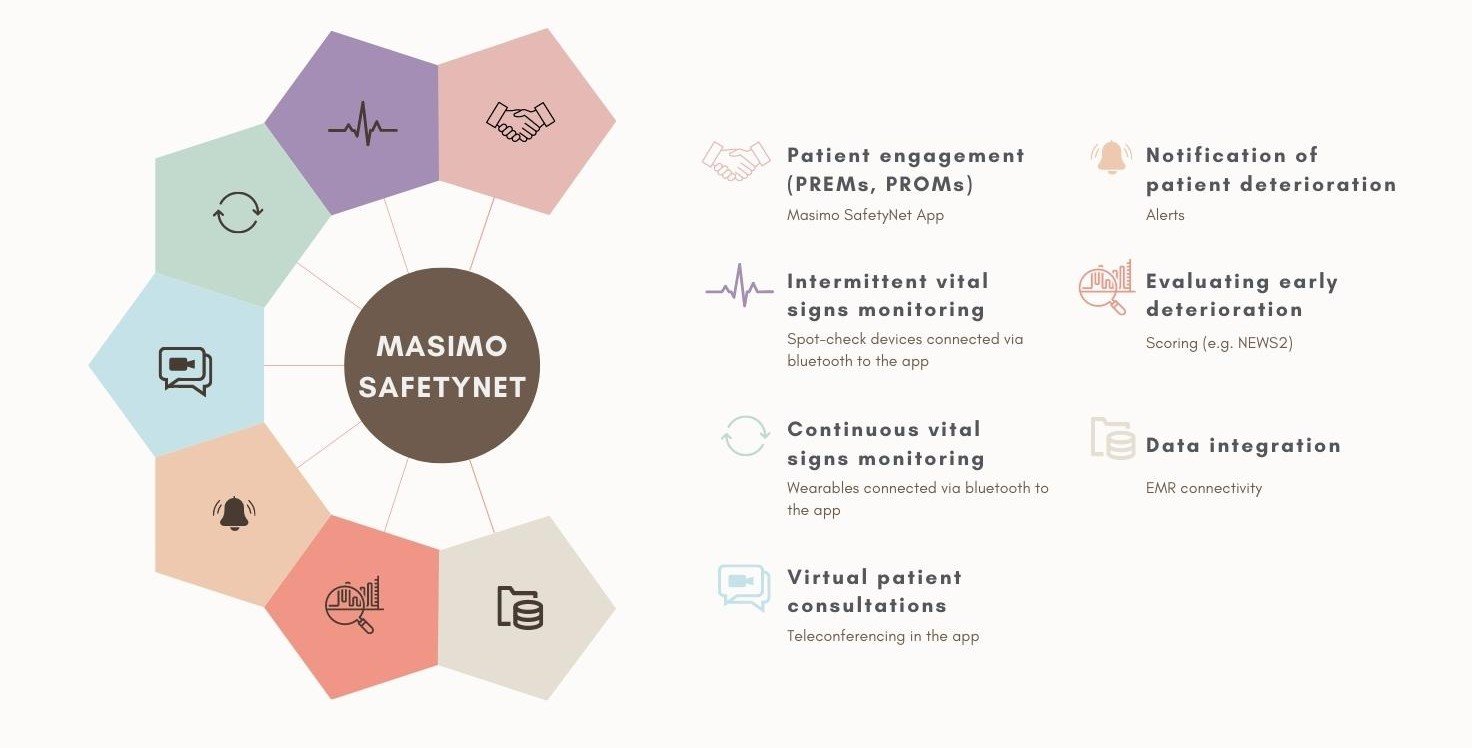
Masimo offers an end-to-end approach to help NHS providers implement Virtual Wards with the Masimo SafetyNet app currently available at no charge for NHS Trusts. The Masimo SafetyNet Virtual Ward solution is an example of a scalable, adaptable Virtual Ward offering, with functionalities summarised below. These functions can be added or removed as the clinical needs change.
Deployment launched across the NHS; contact Masimo to activate your site!
Content provided by Masimo. For more information call +44 (0)1256 479988 or email This email address is being protected from spambots. You need JavaScript enabled to view it..
Integrated care systems must now take the lead in delivering parity for people with mental health problems - Sophie Corlett, Mind Interim CEO
 With 1.8 million people waiting for mental health treatment and no additional investment from the covid recovery funding this year, integrated care systems must now take the lead in delivering parity for people with mental health problems, writes Mind Interim chief executive, Sophie Corlett.
With 1.8 million people waiting for mental health treatment and no additional investment from the covid recovery funding this year, integrated care systems must now take the lead in delivering parity for people with mental health problems, writes Mind Interim chief executive, Sophie Corlett.
The pandemic took a huge toll on the population’s mental health and its impact will be felt for many years to come. We now face a long recession and a cost-of-living crisis which will further drive up need for mental health support, whilst eating into mental health budgets. In addition to an estimated 1.8 million people on waiting lists for mental health treatment, there are 8 million people who would benefit from treatment but do not currently meet clinical thresholds. Pre-pandemic, just over a third of adults with mental health problems and a quarter of children and young people got any treatment at all. As prevalence has grown, particularly amongst children and young people, NHS Long-Term Plan access targets are no longer in step with clinical need. Mind will continue to call for increased funding, including a share of the additional £3.3bn allocated to the NHS in the Autumn Statement. But in the meantime, integrated care systems can and must step up to support the mental health of the population.
We have some reasons to be optimistic. Several amendments were adopted in the final Health and Care Act 2022 that strengthen the hand for mental health. The Act contains an important symbolic commitment to explicitly define “health” to mean both mental and physical health, this decade’s updating of the famed 2012 “parity of esteem” clause. This amendment, first proposed by Lord Simon Stevens, will help to hold the Secretary of State for Health and Social Care accountable to Parliament for spending on mental health.
And, crucially, all integrated care boards are now expected to have a mental health voice at the top table. This is particularly pertinent as so many of the biggest challenges in the NHS right now have a mental health element, from 12-hour waits in accident and emergency departments, to pressures in primary care, to the emotional toll of long waits for elective care. Mental health must be hardwired into pathways across the system.
Early indications are that most of the mental health representatives on integrated care boards are from NHS trusts. This must not mean a focus only on the issues facing providers. ICSs offer an opportunity to finally implement the “radical upgrade in prevention and public health” promised in the Five Year Forward View. There is a strong and growing evidence base for investment to prevent1 those most at risk from developing potentially life-long mental health problems.
Where integrated care partnerships’ mental health strategies are being developed they should have a definitive focus on the wider determinants of mental health such as employment, education and training, housing, transport, and access to green spaces. People with mental health problems are more likely to smoke, misuse substances and to be overweight, so physical public health programmes won’t be effective without a tailored and integrated offer for this population group.
ICSs can use their new freedoms to go further faster where they see the most need, whether that’s scaling up support for children and young people by introducing community-based Early Support Hubs, partnering with the voluntary and community sector to better support racialised and marginalised groups, or working alongside local employers to build trusted partnerships that support people with mental health problems back into the workplace.
The move to a more localised system is not without its risks. Mental health has been neglected for decades and many of the improvements we’ve seen through the Five Year Forward View for Mental Health and the NHS Long-Term Plan have been driven from the centre. We are already hearing of ICS leaders looking to raid ring-fenced Mental Health Investment Standard funding to plug gaps in other parts of the system that have more political focus, such as urgent and emergency services and elective recovery.
Upgrading mental health services to achieve parity was always going to be the work of a generation. Progress is fragile and we cannot afford to slip back into bad habits, such as raising thresholds for mental health care to bail out other parts of the system when unmet need in mental health is so high.
Workforce remains the most pressing challenge. Having led the way in the shift to community-based services, mental health has continued to innovate, creating new roles such as peer support workers to support new models of care. ICS workforce planning is an opportunity to look at the workforce holistically across the NHS, social care and Voluntary, Community and Social Enterprise as well as to look at the best ways local areas can increase support and retain the existing workforce after the challenges of the last few years.
The VCSE is a crucial part of the mental health provider ecosystem, offering innovative and effective community-based services that help to keep people well and avoid hospital admissions. They often support communities that are not well served by statutory services, such as people from racialised communities. They are particularly important for the Community Mental Health Transformation Programme, providing holistic, integrated services that address the wider social determinants of mental health, as well as providing a clinical response.
Integrated Care Systems offer an opportunity to move away from short-term and non-recurrent funding which is difficult and resource intensive to utilise, mitigates against long-term strategic planning and often doesn’t help generate the system change that is needed.
The VCSE are currently under enormous pressure and are picking up the pieces where statutory services not able to offer timely support. They often support people with a high level of risk who can’t get help elsewhere. This is placing a huge strain on them and their staff.
Like all parts of the mental health system, they are facing difficulties with recruitment and retention as salaries are eroded by inflation. This is not helped by NHS commissioners not always passing on the inflation uplift they have received to their VCSE partners and attempts to reduce funding for management costs within contracts. The VCSE can access a different workforce from statutory providers, which is of particular value when there are big workforce challenges for the NHS.
There continue to be practical challenges, for example with the VCSE being able to access NHS data systems, something which risks the safety of service users because the service cannot see their patient records, as well as creating a lot of extra work for them.
The move to Integrated Care Systems has created instability and uncertainly in many areas, disrupting existing relationships and commissioning arrangements. It’s a really mixed picture in terms of how well ICSs are engaging with the VCSE and it can be difficult to know where decisions are being made. We want to see the VCSE treated as equal partners within ICSs. Systems need to consider how they’re engaging with the VCSE more strategically so that they are genuinely co-producing services and ensure they are resourcing this work properly. And simply funding a couple of VCSE engagement roles (recruited by the NHS) isn’t sufficient.
So while the landscape may have shifted again, the task remains the same: to ensure that people with mental health problems can access the help they need, when they need it. ICSs provide the change to get the whole system behind this goal. There is no time to waste.
1. https://www.mentalhealth.org.uk/about-us/news/mental-health-problems-cost-uk-economy-least-gbp-118-billion-year-new-research

Content provided by Sophie Corlett, Mind Interim CEO. For more information please visit www.mind.org.uk.