Sugar Reduction: Preventing Ill Health and Protecting the NHS via Reformulation - Mhairi Brown, Policy and Public Affairs Lead, Graham MacGregor CBE, Chair of Action on Sugar and Action on Salt and Professor Graham MacGregor CBE
 Excess sugar intake is linked to various health issues. There is a causal relationship between sugar intake and tooth decay, which has a large impact on child physical and mental health (1). Oral diseases are the leading reason children aged 5-9 years are admitted to hospital, with 32,140 admissions in 2018-2019 (2). There is also evidence of a link between sugar – particularly in the form of sugar-sweetened drinks - and type 2 diabetes, obesity, liver disease and high LDL cholesterol (1). These health conditions have a huge toll on individuals, families, communities and our overburdened NHS.
Excess sugar intake is linked to various health issues. There is a causal relationship between sugar intake and tooth decay, which has a large impact on child physical and mental health (1). Oral diseases are the leading reason children aged 5-9 years are admitted to hospital, with 32,140 admissions in 2018-2019 (2). There is also evidence of a link between sugar – particularly in the form of sugar-sweetened drinks - and type 2 diabetes, obesity, liver disease and high LDL cholesterol (1). These health conditions have a huge toll on individuals, families, communities and our overburdened NHS.
As a nation, we consume excess sugar and many would likely not realise it. The UK’s food system is dominated by a highly globalised food industry who extensively produce and market processed and nutrient-poor food and drinks – high in fat, sugar and salt (HFSS). These products are cheaper than nutrient-dense products and are at the centre of the billions in profit made by global food companies annually; profits that are often made at the expense of workers’ wages and consumer health (3).
Our food system not only impacts our health, but our environment too, with the conversion of natural ecosystems to crop production or pasture. The production of sugar beet, for example, is causing irreversible damage to soils, with British Sugar being responsible for the removal of hundreds of thousands of tonnes precious of topsoil every year (4).
To address the impact of the UK’s diet on health, the government has implemented numerous policies, including colour-coded front of pack nutrition labels, food and drink procurement guidelines for the public sector and some restrictions on the placement of HFSS products in prominent retail locations. In particular, the government’s reformulation programme is a key policy with the potential for a huge, positive impact on our food system and population health.
UK Sugar Reduction Programme
Reformulation involves food companies improving the nutrition profile of their products, gradually reducing harmful elements such as excess sugar. This removes the barrier of behaviour change or financial considerations from customers, who can continue to buy the same products they always have, but over time they will become healthier. Food companies have gradually reduced salt levels for many years, following the introduction of a Salt Reduction Programme in 2003, and correspondingly, the nation’s blood pressure has reduced alongside a reduction in cardiovascular disease mortality (5). In 2017, the government introduced a Sugar Reduction Programme, with a 20% reduction in sugar levels in certain key contributors to children’s sugar intake expected by 2020, including (6):
- Breakfast cereals
- Yogurts
- Biscuits
- Cakes
- Morning goods (e.g. croissants, English muffins, waffles)
- Puddings
- Ice cream, lollies and sorbets
- Chocolate confectionary
- Sweet confectionary
- Sweet spreads and sauces (e.g. chocolate spread, peanut butter, dessert toppings)
- Juice and milk-based drinks (added 2018)
- Fermented yogurt drinks (added 2019)
PHE proposed that the 20% reduction in sugar content could be achieved by:
- Reformulating products to lower the levels of sugar present
- Reducing the number of calories in, and/or portion size, of products that are likely to be consumed by an individual at one time
- Shifting consumer purchasing towards lower/no added sugar products
With this programme, the UK became one of the first countries to implement sugar reduction targets and WHO Europe was recently tasked with sharing learnings from the UK on sugar and calorie reduction. However, the third progress report, published in 2019, showed that the Sugar Reduction Programme had not achieved the targeted reductions in sugar levels. The fourth and final report (originally due to be published in autumn 2021) has still not been made public so the final state of the programme is unknown and its future unclear.
Factors Impacting Sugar Reduction Progress
There are many factors that may have impacted on the programme’s progress. Targets were set as overall, percentage reductions as opposed to evidence-based and data backed specific targets at the category level (as used in the Salt Reduction Programme). Alongside this, by giving the food industry the option to shift sales to lower or no added sugar products in their portfolios, sugar reduction became a short term marketing opportunity rather than a long term strategic aim. As an example – of which there are many - Mondelez invested heavily in research and marketing for Dairy Milk ‘30% less sugar’, but did not take the risk of reformulating their main product with less sugar (7). However, if provided with motivation, leadership and guidance throughout the process, Mondelez could have successfully reduced the sugar content of many of their products by using the 30% reduced version without advertising this to customers.
Furthermore, sugar reduction was PHE’s flagship policy, but they did not have final say on the structure of the programme as an “executive agency” of the Department of Health and Social Care. PHE’s role was one of providing guidance as opposed to independent and transparent policy making, with the authority to set and enforce strict targets. With PHE’s closure in 2020, the Sugar Reduction Programme lost leadership, credibility and momentum.
By far the leading reason for a lack of progress is that the programme is voluntary, rather than mandatory, supported by legislation. This means that a company can choose to invest as much or as little into reducing sugar in its products as it wants, making full compliance unlikely, as the programme’s progress shows. Indeed, CEO’s of the UK’s major food retailers told the National Food Strategy team – and their nutrition teams have told us directly – that they will not reformulate all products without government legislation, and that “they need a level playing field if they are to start making their products healthier, otherwise the competition will simply move in and undercut them” (8).
The Need for Mandatory Policies
The Soft Drinks Industry Levy provides a useful model for mandated sugar reduction, as it has been instrumental in the reformulation of sugar-sweetened drinks. Due to the tiered structure, companies have been incentivised to reformulate and by 2018, the estimated revenue from the SDIL was downgraded as more than half of companies had reduced the sugar content of drinks since it was announced in March 2016 – the equivalent of 45 million kg of sugar every year - to avoid paying the levy (9). Many drinks companies have the revenue to absorb the cost and continue selling high sugar products, but chose not to.
PHE found that there had been a 43.7% reduction in total sugar content of drinks between 2015 and 2019 (10). Sales of drinks subject to the levy increased, meanwhile, allaying industry fears that the levy would lead to a loss of sales and profit, but the total sugar purchased per household from drinks decreased across all socio-economic groups. Sugar reduction is technically easier to achieve in drinks compared to solid food products, but the SDIL was successful in uniting drinks manufacturers to reformulate to avoid penalties.
What Should Happen Now?
Education is not the answer; despite marketing campaigns like Change4Life and Better You, as well as an app to help make healthier choices, these initiatives have not resulted in sustained or widespread behaviour change (11). The UK needs a Sugar Reduction Programme, and with the expiry of the previous target in 2020, now is the time for the government to implement a comprehensive and mandated sugar reduction programme. The UK’s long-standing Salt Reduction Programme provides an example of an effective public health initiative, launched in 2003 it is still going strong 20 years later. This is because the programme, which comprises specific, data-based targets for a comprehensive range of contributors to the nation’s salt intake, works for the food industry and therefore benefits the nation’s health. Sugar reduction could have that same success if designed in a similar way, with bold government leadership and a strong monitoring framework.

Programme Structure
Building on the model of the salt reduction programme, universally agreed as a well-designed, successful programme by industry and NGOs alike, we need a simple programme with specific, but comprehensive, mandatory upper limits for all contributing categories of sugar to the diet.
The targets can be based on an agreed maximum sugar limit and enforcement could include imposing financial penalties based on individual cases, or a levy applied to a manufacturer in the case of multiple/repeat offences.
In addition to existing categories, additional categories are needed so that all the top contributors to sugar intake are included, including pre-mixed alcoholic drinks, ready meals, sauces, baked beans and bread products.
Governance
The National Food Strategy proposed a statutory duty on sugar (and salt) for all food companies with more than 250 employees – including retailers, restaurant and quick service companies, contract caterers, wholesalers, manufacturers and online ordering platforms – to publish an annual report on the following set of metrics (8):
- Sales of food and drink high in fat, sugar or salt (HFSS) excluding alcohol
- Sales of protein by type (of meat, dairy, fish, plant, or alternative protein) and origin†
- Sales of vegetables
- Sales of fruit
- Sales of major nutrients: fibre, saturated fat, sugar and salt
- Food waste
- Total food and drink sales
This must be implemented by the government (as per its commitment in the Government Food Strategy (12)) to help support governance of the Sugar Reduction Programme, by providing accessible data to government departments and the wider health community to track progress, and ‘name and shame’ companies.
Early Years
Early years (infants and young children aged 0-3 years old) is a black hole of policy making. Despite being a crucial period in a child’s development, to date public health policies fail to cover products marketed for the early years. Products designed for infants and young children, including all products displaying cartoon characters and child friendly packaging, must have strict sugar targets to help ensure infants and young children have access to a range of tastes, rather than products that encourage sweet taste preferences and lead to health issues, particularly tooth decay in the short term.
Benefits of Sugar Reduction
Suboptimal diet is a leading cause of death and disability in the UK and worldwide, costing healthcare services - and the wider economy due to the impact on workforce - billions of pounds each year. Frontier Economics estimated that the total economic impact of obesity alone in 2022 would be £58 billion, accounting for NHS and social care costs, lost productivity, workforce inactivity and welfare payments (13). A similar assessment by McKinsey in 2014 estimated the economic impact of obesity in the UK to be equivalent to 3% of its GDP (14). Therefore, the benefits associated with reducing population sugar intake in the UK are clear, both from a health and an economic standpoint.
Public Health England’s own analysis showed that reducing average energy intake from sugar to 5% over the next 15 years would prevent 3,500 deaths and avoid 173,000 dental caries cases annually, whist also saving the NHS £396m each year (15). More recently, analysis in the National Food Strategy showed that if the Sugar Reduction Programme targets were met, average sugar consumption would reduce by 1 kg to 3.6 kg of sugar per person annually, bringing consumption levels 16% and 83% closer, respectively, to the target intake of 30g sugar per person per day (8). The corresponding reduction in average daily calories per person would be 15-38kcal, which according to experts, could prevent weight gain at a population level (16).
The evidence on the link between excess sugar intake and health has not changed, and our consumption has not gone down. The importance of a healthy, productive population has come into even sharper focus as the UK’s health and care service and economy come under increasing strain. It is vitally important that the government acts now to reduce population sugar intake and thereby protect our health, communities and the NHS.
References
- European Food Safety Authority. Sugar Factsheet. 2021. Available from: https://www.efsa.europa.eu/sites/default/files/2021-07/sugars-factsheet-en.pdf
- NHS Digital. Hospital Admitted Patient Care Activity 2018-19. 2019. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/hospital-admitted-patient-care-activity/2018-19
- Hasnain S, Ingram J, Zurek M. Mapping the UK Food System – a report for the UKRI Transforming UK Food Systems Programme. Environmental Change Institute, University of Oxford, Oxford; Available from: https://www.eci.ox.ac.uk/research/food/downloads/Mapping-the-UK-food-system-digital.pdf
- Feedback. Too Much of a Bad Thing: The use and misuse of UK soil and land to grown sugar. 2019. Available from: https://feedbackglobal.org/wp-content/uploads/2019/11/Too-much-of-a-bad-thing-the-use-and-misuse-of-land-and-soils-to-grow-sugar-Feedback-2019.pdf
- He FJ, Pombo-Rodrigues S, MacGregor GA. Salt reduction in England from 2003 to 2011: its relationship to blood pressure, stroke and ischaemic heart disease mortality. BMJ Open. 2014 Apr 1;4(4):e004549.
- Public Health England. Sugar Reduction: Achieving the 20% A technical report outlining progress to date, guidelines for industry, 2015 baseline levels in key foods and next steps. 2017. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/604336/Sugar_reduction_achieving_the_20_.pdf
- The Grocer. Mondelez unveils Cadbury Dairy Milk 30% Less Sugar. The Grocer. Available from: https://www.thegrocer.co.uk/new-product-development/mondelez-unveils-cadbury-dairy-milk-30-less-sugar/595899.article
- Dimbleby H. National Food Strategy Independent Review: The Plan. 2021. Available from: https://www.nationalfoodstrategy.org/
- HM Treasury. Soft Drinks Industry Levy comes into effect [Internet]. GOV.UK. 2018. Available from: https://www.gov.uk/government/news/soft-drinks-industry-levy-comes-into-effect
- Public Health England. Sugar reduction: report on progress between 2015 and 2019. 2020; Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/984282/Sugar_reduction_progress_report_2015_to_2019-1.pdf
- Croker H, Lucas R, Wardle J. Cluster-randomised trial to evaluate the ‘Change for Life’ mass media/ social marketing campaign in the UK. BMC Public Health. 2012 Jun 6;12(1):404.
- Department for Environment, Food & Rural Affairs. Government food strategy. 2022. Available from: https://www.gov.uk/government/publications/government-food-strategy/government-food-strategy
- Frontier Economics. Estimating the Full Costs of Obesity. 2022. Available from: https://www.frontier-economics.com/media/5094/the-full-cost-of-obesity-in-the-uk.pdf
- McKinsey Global Institute. Overcoming obesity: An initial economic analysis. 2014. Available from: https://www.mckinsey.com/~/media/McKinsey/Business%20Functions/Economic%20Studies%20TEMP/Our%20Insights/How%20the%20world%20could%20better%20fight%20obesity/MGI_Overcoming_obesity_Executive_summary.ashx
- Public Health England. Sugar Reduction The evidence for action. 2015. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/470179/Sugar_reduction_The_evidence_for_action.pdf
- Department of Health and Social Care. Statement of the Calorie Reduction Expert Group. 2011. Available from: https://www. gov.uk/government/publications/statement-of-the-calorie-reduction-expert-group
Contact
Action on Sugar
Action on Sugar is a group of scientific experts concerned with sugar and obesity and its effects on health. It is working to reach a consensus with the food industry and Government over the harmful effects of a high calorie diet, and bring about a reduction in the amount of sugar and fat in processed foods to prevent obesity and type 2 diabetes.
@actiononsugar, actiononsugar.org
Action on Salt
Action on Salt is a group concerned with salt and its effects on health, supported by 23 expert scientific members. Action on Salt is successfully working to reach a consensus with the food industry and Government over the harmful effects of a high salt diet, and bring about a reduction in the amount of salt in processed foods as well as salt added to cooking, and the table, to prevent high blood pressure and cardiovascular disease.
@actiononsalt, actiononsalt.org.uk
Content provided by Mhairi Brown, Policy and Public Affairs Lead & Graham MacGregor CBE, Chair of Action on Sugar and Action on Salt and Professor of Cardiovascular Medicine
Barts and the London, Queen Mary University of London
For more information please visit actiononsugar.org and actiononsalt.org.uk.
The efficacy of the probiotic Symprove as assessed from randomised clinical trials - Ingvar Bjarnason, Department of Gastroenterology, King’s College Hospital
Bacteria emerged from hyperthermophiles about 3.5 billion years ago. They not only adapted to their environment but also changed it creating the oxygen enriched atmosphere that is the pre-requisite for much life on Earth. This apparently altruistic gesture is offset by their destructive nature, as bacteria cause more human deaths than any other single reason, including wars. Man has had to adapt to bacteria and nowhere is this in evidence better than in the gastrointestinal tract. There is a case for considering this interaction as mutualistically beneficial, but there is also a strong case for considering these bacteria as parasitic (1) with limited benefit to the host.
Nevertheless, humans have taken advantage of the properties of some bacteria, for example lactobacillus to preserve foods, mostly dairy products. This gathered momentum with the inclusion of Lactobacillus casei to yogurts in 1930 and this was successfully marketed as conferring a beneficial effect to humans. Most doctors were sceptical to such claims, until efficacy data emerged from randomised clinical trials (RCT). The early trials using lactobacillus and Bifidobacterium in Irritable Bowel Syndrome (IBS) (2, 3) were very convincing.
King’s College Hospital Gastroenterology has been actively involved in the clinical evaluation of Symprove, a non-dairy, liquid probiotic that contains four strains of naturally occurring bacteria: Lactobacillus rhamnosus NCIMB 30174, Lactobacillus plantarum NCIMB 30173, Lactobacillus acidophilus NCIMB 30175 and Enterococcus faecium NCIMB 30176. Here, I will provide an update on the research on its efficacy and highlight the more promising venues for future research.
CLINICAL STUDIES
IBS.
Dr Sisson conducted our first RCT assessing Symprove for management of IBS which is the most common gastrointestinal disorder in developed countries. He studied 186 symptomatic patients, half of whom took Symprove and the other half took a matching placebo (4). Symprove was associated with a significantly greater reductions in the IBS Symptom Severity Scores (SSS) after 12 weeks, mostly due to reduced abdominal pain and improvement in bowel action. Patients with moderate to severe symptoms (IBS- SSS > 175) reported complete resolution of symptoms with Symprove in 26.6% as compared to placebo 14.5% (p = 0.063). Of those who achieved a clinically important difference, defined as a drop of >95 points on the IBS-SSS, 39 (31.5%) vs. 9 (14.5%) achieved this in the probiotic and placebo groups, respectively (p = 0.013). There were no significant improvements in Quality of Life issues.
The fact that this trial was hospital-based means that we included a more severe, problematic or complex IBS cases than the General Practitioner manages. In order to capture the effect of Symprove in less severe cases an independent ‘real life situation’ study was commissioned (5). Participants (n=1246) were recruited through e-mail and social media advertising. These were mostly highly educated, non-smoking, health-conscious women with IBS. Over 90% reported improvements (‘completely resolved’ or ‘some positive difference’) in IBS or IBS-like symptoms, including abdominal pain (p<0.001), bloating (p<0.001), urgency to defecate (p<0.001) and bowel habit satisfaction (p<0.001). At face value this indicates, as is the case in many disease, that efficacy is markedly greater in milder disease.
Given this I now routinely advocate a holistic approach to treatment of IBS. This involves dietary assessment with implementation of a variety of food exclusions such as the low-FODMAP diet, the use of Symprove and an appropriate referral to a psychiatrist who is interested in the subject matter. About 70% of patients may be expected to gain significant benefit from this approach, which far greater than seen with traditional drug treatment.
DIVERTICULAR DISEASE
Colonic diverticular disease (DD) i.e. pouch-like bulging of the colonic, predominantly the sigmoid wall, is evident in approximately 40% and 70% of people aged over 60 and 80 years, respectively. About 25% experience an episode of acute diverticulitis. Acute diverticulitis is perceived to be a ‘surgical’ disease, but most patients recover without an operation. However, many such patients consequentially develop problematic IBS like symptoms.
Conventional treatment includes high fibre supplements, anti-diarrhoeals or anti-obstipants that lead to roller-coaster changes in bowel habits and anti-spasmotics. These patients are now share managed by colorectal surgeons and Gastroenterologists in dedicated “Diverticular Disease Clinics” at King’s College Hospital.
We assessed the efficacy of Symprove by itself (without other specific treatments) in a RCT involving 120 adult patients with moderate-to-severe chronic, non-acute symptomatic diverticular disease (6).
Symprove taken over 12 weeks was associated with significant improvements in diarrhoea, constipation mucorrhoea and back pain. Patients abdominal pain decreased in both groups, but did not reach a statistical significance (p = 0.11).
Three patients on Symprove and eitght on placebo developed diverticulitis during the study (p = 0.19). Given this we now advocate Symprove for these patients, but there is clearly the potential to consider further studies.
INFLAMMATORY BOWEL DISEASE (IBD)
There was a hint from the above studies that Symprove had subtle anti-inflammatory properties. We designed a study assessing faecal calprotectin, a quantitative marker of intestinal inflammation, before and after four weeks of Symprove v placebo in asymptomatic patients with ulcerative colitis (n=81) and Crohn’s disease on minimal medical treatment (7). This represents a small group of patients with IBD who have a more benign course of disease than most. In short calprotectin levels were significantly (p < 0.015) reduced in the patients with ulcerative colitis receiving the probiotic as opposed to placebo, demonstrating an anti-inflammatory effect. No significant differences were seen in Crohn’s Disease. This was not a clinical outcome trial, but suggests that some patients with ulcerative colitis may benefit from taking Symprove.
POTENTIAL BENEFITS
COVID-19
The pan-epidemic due to COVID-19 has affected millions of people and accounts for about 160, 000 premature deaths in the UK at present. The most severe disease requires intensive care treatment. About 50% of such patients die and many of the survivors have a delayed recovery, requiring intensive prolonged rehabilitation with symptoms reminiscent of the chronic fatigue syndrome (8).
The gastrointestinal tract has been the focus of some research during this epidemic. 30- 50% infected patients shed the virus in stool (9-11) and many have a ‘gastroenteritis’ like illness (12, 13). It has been suggested that the gastrointestinal involvement plays an important role in increasing the severity of complications of the infection (14-16).
There has been one open uncontrolled study of a probiotic in COVID-19 patients. D’Ettorre et al (17)assessed the effect of Sivomixx, a multistrain freeze-dried formulation of lactic acid- and bifido-bacteria, in 28 patients with COVID-19 receiving the probiotic as compared with 42 control patients. The probiotic was associated with resolution of diarrhoea within three days (94%) as compared with 30% for those not on probiotics p < 0.001. There was a significantly more rapid resolution of composite symptoms (tiredness, headache, myalgia and dyspnoea) in the probiotic treatment evident within 48 and 72 hours (p<0.001). On day seven 98% of the probiotic group had improvements in the symptom severity as compared to 40% in the patients not receiving the probiotic supplement (p < 0.001). Furthermore, on day seven there was an eightfold decrease in the requirement of respiratory support in the probiotic group (p = 0.01).
If similar results were evident in RCT then this treatment would revolutionise the management of severe Covid.
PARKINSON’S DISEASE.
Twenty years ago there was a neurological consensus that Parkinson’s Disease was a localised brain disease with a prominent genetic disease basis with some environmental triggers in the minority of cases. Then the idea that it was a more generalised disease emerged (18) and the Dobbs’ team launched an integrated research program into a gut – CNS association (19-21). To make a long story short, they found that eradication of H pylori not only halted but reversed brady/hypokinesia while treatment failure led to further deterioration (22-24). This work even suggested an importance for H suis (25, 26). However, H pylori treatment success was associated with small intestinal bacterial overgrowth (SIBO) (27, 28) with deterioration of symptoms. Introduction of a maintenance laxative in these cases shows plateauing of year-on-year increase in rigidity (29, 30). These findings conform to the idea that intestinal dysbiosis contributes to certain facets of Parkinson’s disease. Symprove has been suggested as an adjunct treatment for Parkinson’s disease and some trials are completed but the results are unknown and further funding has been sought for multi-centre trials.
FURTHER POTENTIAL
It is increasingly recognised that the intestinal microbiome is variously disturbed in several clinical conditions and disease. Such findings do not establish a cause and effect relationship. Indeed there is no certainty that probiotics will be of benefit in these conditions and it will be necessary to demonstrate efficacy in adequately designed clinical trials.
- Bjarnason I, Rainsford KD. NSAID-enteropathy and intestinal microbes. . Inflammopharmacology 2021 Feb;29(1):1-4 doi: 101007/s10787-020-00766-8 Epub 2020 Oct 15 PMID: 33058017.
- O’Mahony L, McCarthy J, Kelly P, et al. Lactobacillus and bifidobacterium in irritable bowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterology. 2005;126:541-51.
- Whorwell PJ, Altringer L, Morel J, et al. Efficacy of an encapsulated probiotic Bifidobacterium infantis 35624 in women with irritable bowel syndrome. Am J Gastroenterol. 2006;101:1581-90.
- Sisson G, Ayis S, Sherwood RA, et al. Randomised clinical trial: A liquid multi-strain probiotic vs. placebo in the irritable bowel syndrome--a 12 week double-blind study. Aliment Pharmacol Ther. 2014;40:51-60.
- Rudland S BI. A multi-strain liquid probiotic in the management of irritable bowel syndrome: A real-world evidence study. Submitted. 2021.
- Kvasnovsky CL, Bjarnason I, Donaldson AN, et al. A randomized double-blind placebo-controlled trial of a multi-strain probiotic in treatment of symptomatic uncomplicated diverticular disease. Inflammopharmacology. 2017;May 20. doi: 10.1007/s10787-017-0363-y.
- Bjarnason I, Sission G, Hayee B. A randomised, double-blind, placebo-controlled trial of a multi-strain probiotic in patients with asymptomatic ulcerative colitis and Crohn’s disease. Inflammopharmacology. 2019;27:465-73.
- Yeoh YK, Zuo T, Lui GC, et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut. 2021;70:698-706.
- Pamplona J, Solano R, Soler C, et al. Epidemiological approximation of the enteric manifestation and possible fecal-oral transmission in COVID-19: a preliminary systematic review. Eur J Gastroenterol Hepatol 2020 Sep 17 doi: 101097/MEG0000000000001934.
- Parasa S, Desai M, Thoguluva Chandrasekar V, et al. Prevalence of Gastrointestinal Symptoms and Fecal Viral Shedding in Patients With Coronavirus Disease 2019: A Systematic Review and Meta-analysis. JAMA Netw Open 2020 Jun 1;3(6):e2011335 doi: .
- Hajifathalian K, Mahadev S, Chwartz RE, et al. SARS-COV-2 infection (coronavirus disease 2019) for the gastrointestinal consultant. World J Gastroenterol. 2020;26:1546-53.
- Ghoshal UC, Ghoshal U, Dhiman RK. Gastrointestinal and Hepatic Involvement in Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Review. J Clin Exp Hepatol 2020 Jun 11 doi: 101016/jjceh202006002.
- Galanopoulos M, Gkeros F, Doukatas A, et al. COVID-19 pandemic: Pathophysiology and manifestations from the gastrointestinal tract. World J Gastroenterol,. 2020;26:4579-88.
- Pan L, Mu , Yang P, et al. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am J Gastroenterol. 2020;115:766-73.
- Hoel H, Heggelund L, Reikvam DH, et al. Elevated markers of gut leakage and inflammasome activation in COVID-19 patients with cardiac involvement. J Intern Med 2020 Sep 25 doi: 101111/joim13178.
- van der Lelie D, Taghavi S. COVID-19 and the Gut Microbiome: More than a Gut Feeling. mSystems 2020 Jul 21;5(4):e00453-20 doi: 101128/mSystems00453-20.
- d’Ettorre G, Ceccarelli G, Marazzato M, et al. Challenges in the Management of SARS-CoV2 Infection: The Role of Oral Bacteriotherapy as Complementary Therapeutic Strategy to Avoid the Progression of COVID-19. Front Med (Lausanne) 2020 Jul 7;7:389 doi: 103389/fmed202000389 eCollection 2020.
- Braak H, Rub U, Gai WP, et al. Idiopathic Parkinson’s disease: Possible routes by which vulnerable neuronal types may be subject to neuroinvasion by an unknown pathogen. J Neural Transm. 2003;110:517-36.
- Dobbs SM, Dobbs RJ, Weller C, et al. Link between Helicobacter pylori infection and idiopathic parkinsonism. Med Hypotheses. 2000;55:93-8.
- Dobbs RJ, Dobbs SM, Weller C, et al. Helicobacter hypothesis for idiopathic parkinsonism: before and beyond. Helicobacter. 2008;13:309-22.
- Weller C, Oxlade N, Dobbs SM, et al. Role of inflammation in gastrointestinal tract in aetiology and pathogenesis of idiopathic parkinsonism. FEMS Immunol Med Microbiol. 2005;44:129-35.
- Dobbs SM, Dobbs RJ, Weller C, et al. Differential effect of Helicobacter pylori eradication on time-trends in brady/hypokinesia and rigidity in idiopathic parkinsonism. Helicobacter. 2010;15:279-94.
- Dobbs RJ, Dobbs SM, Weller C, et al. Role of chronic infection and inflammation in the gastrointestinal tract in the etiology and pathogenesis of idiopathic parkinsonism. Part 1: eradication of Helicobacter in the cachexia of idiopathic parkinsonism. Helicobacter. 2005;10:267-75.
- Bjarnason IT, Charlett A, Dobbs RJ, et al. Role of chronic infection and inflammation in the gastrointestinal tract in the etiology and pathogenesis of idiopathic parkinsonism. Part 2: response of facets of clinical idiopathic parkinsonism to Helicobacter pylori eradication. A randomized, double-blind, placebo-controlled efficacy study. Helicobacter. 2005;10:276-87.
- Blaecher C, Smet A, Flahou B, et al. Significantly higher frequency of Helicobacter suis in patients with idiopathic parkinsonism than in control patients. Aliment Pharmacol Ther. 2013;38:1347-53.
- Augustin AD, Savio A, Nevel A, et al. Helicobacter suis Is Associated With Mortality in Parkinson’s Disease. Front Med (Lausanne) 2019 Aug 28;6:188 doi: 103389/fmed201900188 eCollection 2019.
- Dobbs RJ, Charlett A, Dobbs SM, et al. Leukocyte-subset counts in idiopathic parkinsonism provide clues to a pathogenic pathway involving small intestinal bacterial overgrowth. A surveillance study. Gut Pathog 2012 Oct 19;4(1):12 doi: 101186/1757-4749-4-12.
- Dobbs SM, Charlett A, Dobbs RJ, et al. Antimicrobial surveillance in idiopathic parkinsonism: indication-specific improvement in hypokinesia following Helicobacter pylori eradication and non-specific effect of antimicrobials for other indications in worsening rigidity. Helicobacter. 2013;18:187-96.
- Tucker RM, Ryan S, Hayee BH, et al. Distinctive Pathophysiology Underlying Constipation in Parkinson’s Disease: Implications for Cognitive Inefficiency. J Clin Med 2020 Jun 19;9(6):1916 doi: 103390/jcm9061916.
- Augustin AD, Charlett A, Weller C, et al. Quantifying rigidity of Parkinson’s disease in relation to laxative treatment: a service evaluation. Br J Clin Pharmacol. 2016;82:441-50.
Content provided by Professor Ingvar Bjarnason, Department of Gastroenterology, King’s College Hospital, Denmark Hill, London SE5 9PJ
Tel: 07784 589003
Email: This email address is being protected from spambots. You need JavaScript enabled to view it.
How can Primary Care Networks utilise their estates to support the delivery of improved health outcomes and support healthcare led regeneration? - AA Projects
The health and social care sectors are seeing unprecedented challenges, which is putting pressure on our systems to improve both quality and efficiency whilst improving patient outcomes in the face of increasing demand.
It is estimated that over 15 million people in England alone are living with a long-term condition1 such as hypertension, depression, asthma, or diabetes. These types of conditions account for around 50% of all GP appointments2 and a high percentage of stays in hospital beds. This number will continue to increase as our population ages and complex health conditions increase, by 2030 it is anticipated that the number of people aged over 75 will increase by over 50%3.
The drivers for change within health and social care don’t stop at demographics, these drivers are well documented and include:
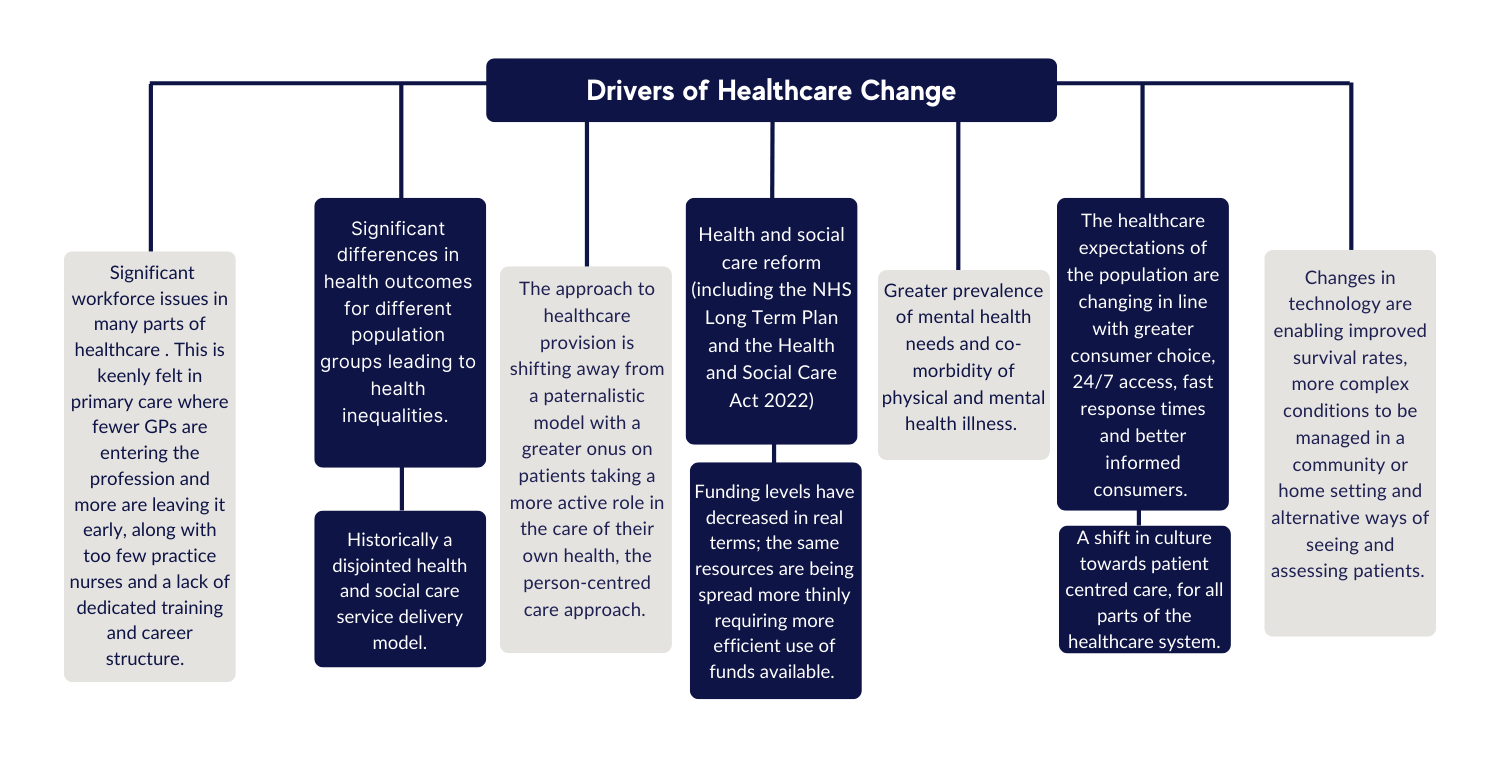
Figure 1 - Drivers of Healthcare change
General practice is the first point of call for most users of the NHS, therefore the above drivers result in a huge impact on their services and the premises that accommodate them. As a consequence, increased demand, the need to deliver the Primary Care Network (PCN) contract, along with ever expanding services, has left many GP practices across the country struggling to provide essential primary care services because of inadequate premises.
This means that the need for primary care providers to have access to and operate from modern, efficient buildings, equipped with the latest technologies that are reliable and well-maintained, with the capacity to cope with future demands has never been more important.
Why is estate planning so important for primary care and networks?
Often premises issues are considered after service redesign discussions have concluded and the limitations of unsuitable premises are therefore not recognised early enough.
This can lead to primary care and community estate being a blocker rather than an enabler to moving more care out of an acute setting.
This means that the importance of estate planning at a PCN level cannot be underestimated, enabling networks and general practice to work with partners to deliver a range of extended community-based services in optimal care settings closer to people’s homes. This would allow primary care and PCNs to respond to the changing needs of their local population and improve patient outcomes.
The principles of estate planning and developing a strategy are universal across sectors and organisation, consisting of a four-stage approach, which asks the following questions of the organisation:
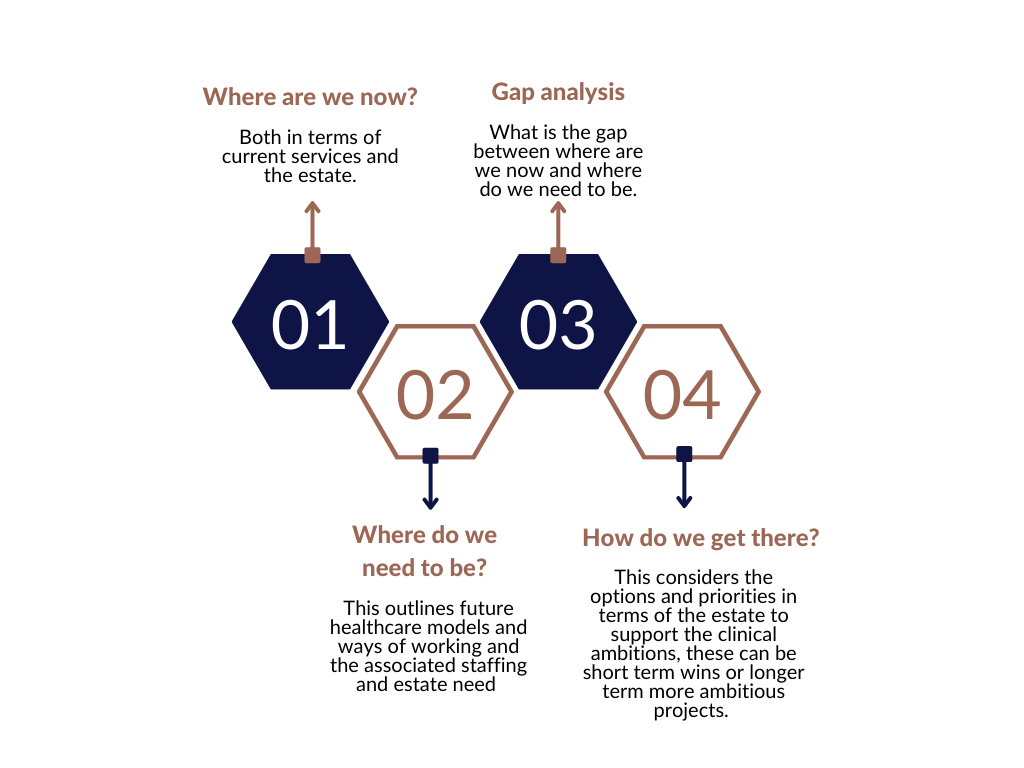
Figure 2 - The four-stage estate planning approach
Some of the longer-term solutions for PCN or systems can involve significant investment, therefore it is crucial that prior to jumping to new build solutions that all other options are considered. This includes maximising the utilisation of current suitable estate and working with partners across the public sector to ensure that all public sector assets are appraised. This can lead to some shorter term, quick win solutions for general practice and networks.
In some areas there is likely to be a need to review more radical longer-term solutions in order to support the delivery of new models of care, which are people-centred, focusing on a holistic approach to people’s well-being including education and health prevention. This may involve the development of new premises or repurposing of existing estate.
When looking at developments of these types of facilities it is clear that there are key considerations:
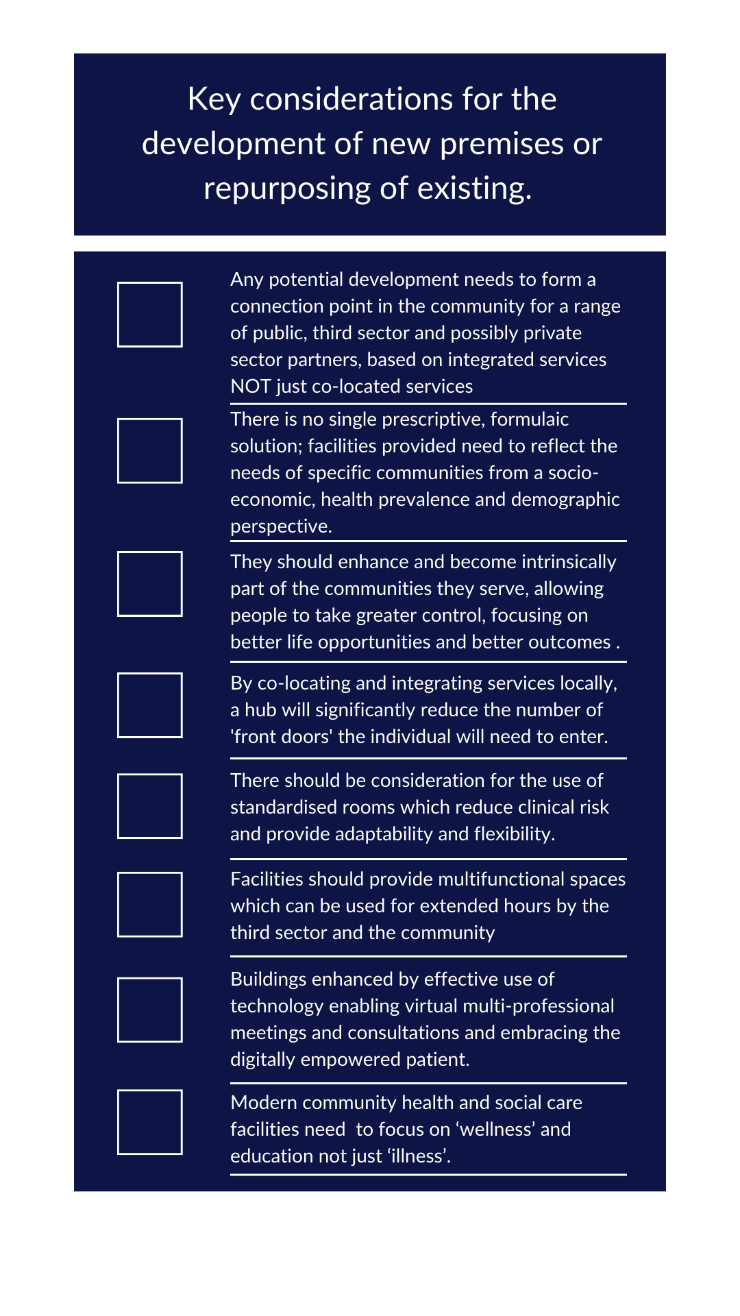
Figure 3 - Key considerations for healthcare developments
How can well planned health estate support regeneration?
The location and accessibility of public sector assets including health facilities is critical when planning for the future. Faculties need to be well-located to ensure equitable access for all and inclusive design-meaning everyone can use service and facilities safely, easily and with dignity. The need for public sector buildings in which to deliver new service models can also act as a significant catalyst for change in a community, spearheading investment and potentially regeneration.
This opportunity for future healthcare developments to support regeneration in communities could be pivotal in reimagining what our high streets look like. Through the NHS Reset campaign, the NHS Confederation and Power to Change are working with national and local leaders from a broad range of sectors to understand the challenges facing the high street and the opportunities to rethink the critical role the health sector can play as places look to recover economically and socially from COVID-19.
There are significant benefits which could be realised by building health into our declining streets. Not only can it play an important role in addressing health inequalities, offer additional capacity for health service delivery and encourage healthier lifestyles, but can also attract greater footfall onto the local high street, which in many places have been decimated by the growth of out-of-town retail centres and internet shopping. This can lead to more people visiting high streets who may not previously have done so, either as staff members who work in health and social care or people accessing services, creating more vibrant spaces with potential for change in both ethos and diversity.
Looking to our high streets and creating multi-functional town centres that are a focal point for health, both in terms of creation and treatment promotes prosperity, improves safety as well as encourages interaction.
Due to high streets generally being more accessible to people without cars who utilise public transport, cycle or walk, improved health and public sector services at the heart of communities should also make a wider range of health and care services more accessible, increase patient and customer engagement and lead to improvements in health outcomes and the wider determinants of health.
With integrated and joined-up public sector partner working, along with well-designed inclusive facilities located in the right place, an ethos of ‘every contact counts’ can easily be implemented; where all encounters are seen as an opportunity for a brief intervention to support improved lifestyle choices or to allow underlying issues such as debt or housing issues to be addressed.
Implementing high-quality built environment interventions is one way the health and social care sector can address the current disjointed service delivery model and move towards the development of places that are designed for public interaction, bringing the public health and economic gains that come with good quality high-street design to the forefront of local and national stakeholder attention.
Without action, Primary Care Networks will miss out on implementing cost effective built environment solutions that not only make economic sense but also work to provide local communities with clear ‘building blocks’ for health.
An excellent example is Limelight which is an award-winning health and wellbeing hub located in the heart of Old Trafford, Greater Manchester. Part of Trafford Housing Trust, Limelight offers a wide range of facilities, community activities, and health social care and local authority services, as well as extra care apartments.
The key focus is on the local community and Limelight being a the hub of Old Trafford, where people can come to meet, eat, celebrate, collaborate, learn and grow.

Figure 4 - Limelight. Old Trafford, Greater Manchester

Figure 5 - The current disjointed service delivery model vs integrated service delivery
References
1 Long-term conditions and multi-morbidity | The King’s Fund (kingsfund.org.uk)
2 Long-term conditions and multi-morbidity | The King’s Fund (kingsfund.org.uk)
3 UK population aged over 75 (millions) | The Nuffield Trust

Content provided by Jonathan Turner, AA Projects. For more information please visit www.aaprojects.co.uk or email This email address is being protected from spambots. You need JavaScript enabled to view it..




 The delivery of care in England has seen its biggest shake-up in recent history following implementation of the new Health and Care Act [July 2022]. The act is an acknowledgement by healthcare leaders that responding to ever increasing demands for healthcare requires a new and more connected approach. Leading this change are 42 new Integrated Care Systems [ICS], which together with their boards and statutory partnerships have responsibility for the commissioning and delivery of health and care services across the NHS.
The delivery of care in England has seen its biggest shake-up in recent history following implementation of the new Health and Care Act [July 2022]. The act is an acknowledgement by healthcare leaders that responding to ever increasing demands for healthcare requires a new and more connected approach. Leading this change are 42 new Integrated Care Systems [ICS], which together with their boards and statutory partnerships have responsibility for the commissioning and delivery of health and care services across the NHS.



