The CompreHensive geriAtRician-lead MEdication Review (CHARMER) hospital deprescribing intervention: What it means for primary care - Sion Scott, Lecturer in Behavioural Medicine & Debi Bhattacharya, Professor of Behavioural Medicine, University of Leices
Background
The National Overprescribing Review (NOR) estimates that 10% of medicines prescribed are inappropriate either because they are unnecessary or harmful(1). Deprescribing is the process of a healthcare professional working in partnership with the patient and/or caregiver to identify and discontinue inappropriate medicines(2). Deprescribing may either be ‘reactive’, in response to medication-related harm that has already happened, or ‘proactive’, in order to prevent medication-related harm from happening as illustrated by Figure 1.
Inappropriate medicines are associated with a range of adverse outcomes including morbidity, hospitalisation and mortality(3). Systematic reviews of randomised controlled trials demonstrate that proactive deprescribing is safe and associated with positive patient and health system outcomes(4–6). Accordingly, there is a need to embed proactive deprescribing into routine practice to prevent harm and unnecessary health resource use.
The NOR advocates a system-wide approach to tackling overprescribing; primary care setting has responded with significant policy and practice change(1). For example, the introduction of structured medication reviews in 2020 which require primary care organisations to target patients who are at high risk of being prescribed unnecessary or harmful medicines(7).
An admission to hospital is another opportunity to identify and deprescribe inappropriate medicines, complementing the strategies in primary care(8). An estimated 1 in 2 people aged ≥65 years admitted to hospital are prescribed at least one medicine that should be deprescribed(9). However, research undertaken by the CHARMER team demonstrates that virtually no proactive deprescribing occurs during a hospital admission(10). This is despite over 9 in 10 older hospital patients and caregivers stating that they would be willing to have a medicine deprescribed during a hospital admission(11).
There are a number of compelling reasons to bring the hospital setting into the fold to support tackling overprescribing including the presence of geriatricians and pharmacists who are experts in older people and medicines respectively, and the facility to intensively monitor a patient’s response to deprescribing(8). However, as with all healthcare settings, there are a number of barriers and enablers to proactive deprescribing in hospital that require addressing before it becomes routine practice.

Figure 1: A comparison of reactive and proactive deprescribing
The CHARMER intervention
CHARMER is a deprescribing intervention aimed at increasing proactive deprescribing undertaken by geriatricians and pharmacists in hospitals in England. Five years of funding was awarded by the National Institute for Health and Care Research (NIHR) to develop the CHARMER intervention and test its effectiveness and cost-effectiveness. The CHARMER intervention does not direct clinical decision-making; it is designed to address the practical and social factors that geriatricians and pharmacists say hinder proactive deprescribing in hospital. For example, one barrier is that geriatricians and pharmacists feel that patients may be resistant to having a medicine deprescribed in hospital, despite evidence to the contrary(11). CHARMER therefore includes a component designed to address this barrier; video case studies demonstrating geriatricians successfully navigating deprescribing consultations with patients and caregivers. Figure 2 provides a summary of the five components of the CHARMER intervention.

Figure 2: Five components of the CHARMER intervention
The CHARMER feasibility study was completed in 2022 and concluded that implementing the intervention in NHS hospitals and conducting a definitive trial was feasible(12). 1st February 2024 marked the commencement of the CHARMER definitive trial. The trial involves 24 acute hospitals listed in Figure 3, over 100 geriatricians and pharmacists and 24,000 patients admitted to Older People’s Medicine wards. The primary outcome measure for the trial is a reduction in 90-day hospital readmission.
What CHARMER means for primary care
Whilst CHARMER is a hospital-based intervention, any change in hospital deprescribing activity will impact on other settings within the healthcare system, principally primary care. Early in the CHARMER programme, a Primary Care Advisory Group (PCAG) was established including membership from the following:
- Medical directors and clinical pharmacists of Integrated Care Systems
- Directors and Prescribing Leads of Integrated Care Systems (ICSs)
- Directors of Primary Care Networks (PCNs)
- Commissioners of Primary Care Medicine Services
- Senior GPs and pharmacists with a role or interest in medicines optimisation
The PCAG provides strategic oversight by identifying and advising on any potential barriers and enablers in primary care relevant for successfully implementing CHARMER and maximising return to the healthcare system. Communication at the transfer of care, maintenance and monitoring of deprescribing post-discharge have been extensively considered by the PCAG and CHARMER team.
If the CHARMER intervention is effective, primary care teams will see patients being discharged from hospital with more medicines deprescribed than historical rates. Some deprescribing will not require any further action from primary care teams, however clear communication including a rationale for deprescribing in the discharge communication is essential to prevent uncertainty and potential re-prescribing owing to a gap in information. There may be instances where deprescribing has happened in hospital which requires a degree of minoring by primary care, or where gradual deprescribing has been initiated in hospital which requires primary care to take over. This is similar to situations where medicines are started in hospital that require follow-up by primary care. In both instances, in addition to the aforementioned communication, hospital teams must ensure that the information provided in the discharge communication is comprehensive and supports primary care colleagues to maintain hospital-initiated deprescribing.
There is significant variation in transfer of care between hospitals and primary care across the country and this is likely to be reflected in the CHARMER trial. This presents both a risk and an opportunity to CHARMER. Poor transfer of care increases the chances of failing to realise the gains from successful deprescribing in hospital. Transfer of care that facilitates maintenance of deprescribing and ongoing monitoring where necessary is imperative to realising any benefits from CHARMER in addressing national overprescribing.
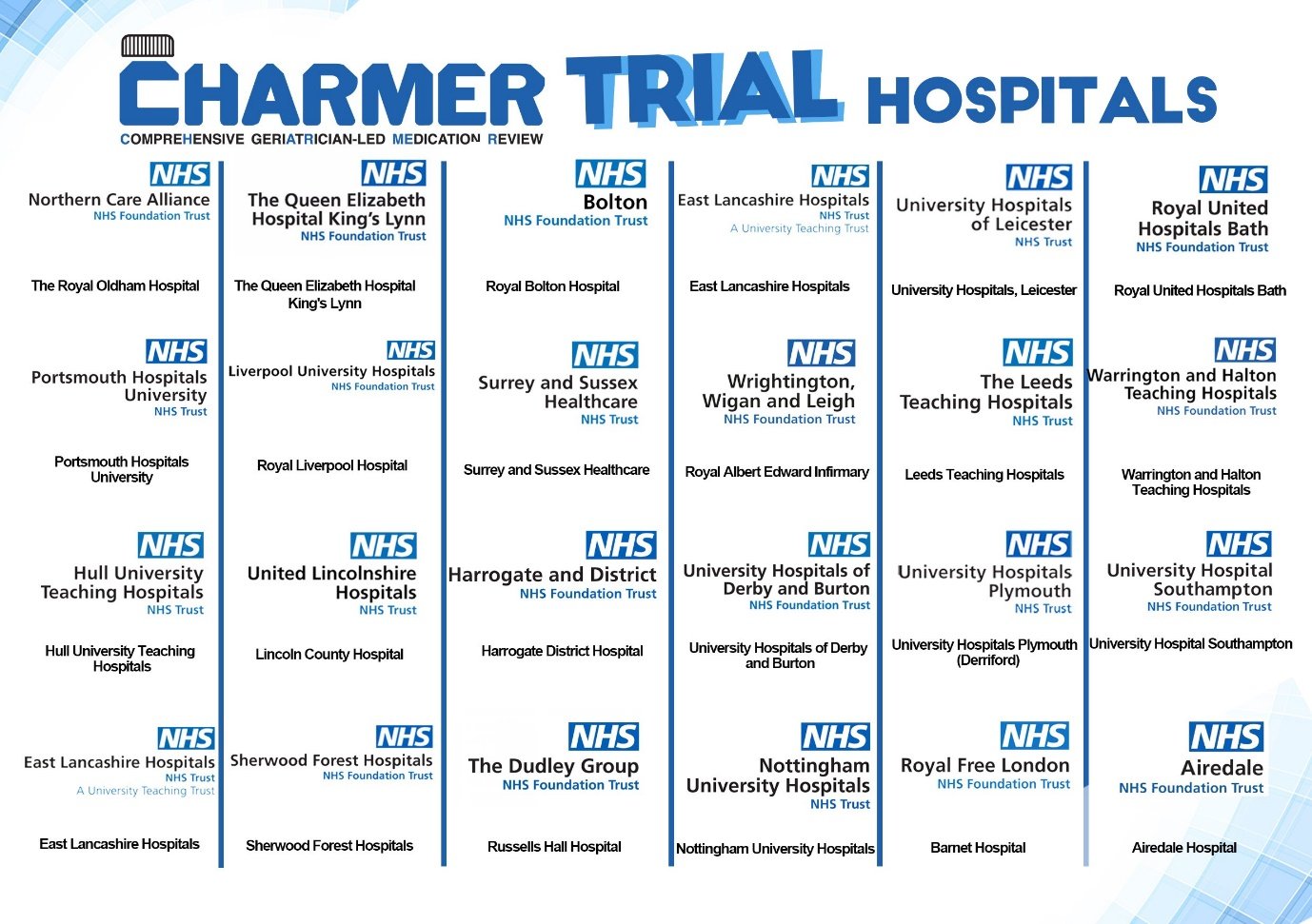
Figure 3: The 24 hospitals participating in the CHARMER trial
Primary care investing in maintaining hospital initiated deprescribing can help foster a system-wide approach to tackling overprescribing in the NHS and maximise the benefits of CHARMER. All primary care colleagues for whom a patient is discharged from a CHARMER hospital and has been enrolled in the trial will be invited to provide feedback on the impact of the intervention. Discharge communication will be annotated to inform primary care of the patient’s enrolment in the trial and will include an invitation to provide feedback The CHARMER team are interested in all feedback its impact, either positive or negative. In the event that you are likely to receive patients who are discharged from the care of one of the CHARMER hospitals, please look out for the invitation in the discharge communication.
For more information about the CHARMER programme of research, visit www.charmerstudy.org, email This email address is being protected from spambots. You need JavaScript enabled to view it. and follow us on X: @CHARMER_Study.
References
- Good for you, good for us, good for everybody: A plan to reduce overprescribing to make patient care better and safer, support the NHS, and reduce carbon emissions [Internet]. Department of Health and Social Care; 2021 [cited 2021 Dec 21]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1019475/good-for-you-good-for-us-good-for-everybody.pdf
- Woodward MC. Deprescribing: achieving better health outcomes for older people through reducing medications. J Pharm Pract Res. 2003;33(4):323–8.
- Spinewine A, Schmader KE, Barber N, Hughes C, Lapane KL, Swine C, et al. Appropriate prescribing in elderly people: how well can it be measured and optimised? The Lancet. 2007;370(9582):173–84.
- Bloomfield HE, Greer N, Linsky AM, Bolduc J, Naidl T, Vardeny O, et al. Deprescribing for community-dwelling older adults: a systematic review and meta-analysis. J Gen Intern Med. 2020;35(11):3323–32.
- Page AT, Clifford RM, Potter K, Schwartz D, Etherton-Beer CD. The feasibility and effect of deprescribing in older adults on mortality and health: a systematic review and meta-analysis. Br J Clin Pharmacol. 2016;82(3):583–623.
- Thillainadesan J, Gnjidic D, Green S, Hilmer SN. Impact of deprescribing interventions in older hospitalised patients on prescribing and clinical outcomes: a systematic review of randomised trials. Drugs Aging. 2018;35(4):303–19.
- Network Contract Directed Enhanced Service Structured medication reviews and medicines optimisation: guidance [Internet]. [cited 2022 Oct 6]. Available from: https://www.england.nhs.uk/wp-content/uploads/2021/03/B0431-network-contract-des-smr-and-mo-guidance-21-22.pdf
- Scott S, Twigg MJ, Clark A, Farrow C, May H, Patel M, et al. Development of a hospital deprescribing implementation framework: a focus group study with geriatricians and pharmacists. Age Ageing. 2020;49(1):102–10.
- Gallagher P, Lang PO, Cherubini A, Topinková E, Cruz-Jentoft A, Montero Errasquín B, et al. Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitals. Eur J Clin Pharmacol. 2011;67(11):1175–88.
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Deprescribing admission medication at a UK teaching hospital; a report on quantity and nature of activity. Int J Clin Pharm. 2018;40(5):991–6.
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Attitudinal predictors of older peoples’ and caregivers’ desire to deprescribe in hospital. BMC Geriatr. 2019;19(1):1–11.
- Scott S, Atkins B, Martin-Kerry JM, Pritchard M, Alldred DP, Clark AB, et al. CompreHensive geriAtRician-led MEdication Review (CHARMER): protocol for a feasibility study of a hospital deprescribing behaviour change intervention. BMJ Open. 2023 Aug 1;13(8):e075795.
Content provided by Sion Scott, Lecturer in Behavioural Medicine, University of Leicester & Debi Bhattacharya, Professor of Behavioural Medicine, University of Leicester
For more information visit www.charmerstudy.org, or email This email address is being protected from spambots. You need JavaScript enabled to view it..
Glenholme Healthcare Group improves efficiency with Workforce.com
 Glenholme Healthcare Group is a distinguished care provider with nearly 3 decades of delivering exceptional care throughout England. With the rapid growth of their care services which now include supported living, residential care, and senior living, Workforce.com has helped them streamline rota building, reduce manual administrative tasks, and enhanced the overall staff experience.
Glenholme Healthcare Group is a distinguished care provider with nearly 3 decades of delivering exceptional care throughout England. With the rapid growth of their care services which now include supported living, residential care, and senior living, Workforce.com has helped them streamline rota building, reduce manual administrative tasks, and enhanced the overall staff experience.
Initially focusing on residential support for adults with mental health conditions, Glenholme has expanded its workforce from 200 to 870 employees in only 4 years and has homes spanning from Blackpool to Brighton. Glenholme provides genuinely personalised support for the elderly and those with nursing care needs and dementia, as well as adults with severe learning disabilities and a variety of complex needs.
The challenge
Prior to Workforce.com, the process of creating rotas at Glenholme Healthcare was time-consuming, taking approximately 4 hours per week to complete. The existing system was deemed clunky and difficult to use, resulting in limited adoption by staff and lost time for front-line managers.
Additionally, the care home struggled with a lack of visibility into its business operations, making it challenging to have a comprehensive overview of staff availability, leave balances, and overall scheduling. Overcoming these challenges and implementing an improved workforce management system became crucial for Glenholme to streamline operations, enhance user experience, and ensure efficient management of staff.
The solution
Glenholme went searching for a cloud-based system that could solve their challenges and scale with their business growth. After conducting a thorough market review, Glenholme decided to invest in Workforce.com due to its intuitive design, product functionality and easy implementation process.
"Implementation is a relatively easy process and the support team really helped us and was a great experience."
- James Perkins, Finance Manager at Glenholme Healthcare Group
The results
 Saving time on rota creation & manual admin
Saving time on rota creation & manual admin
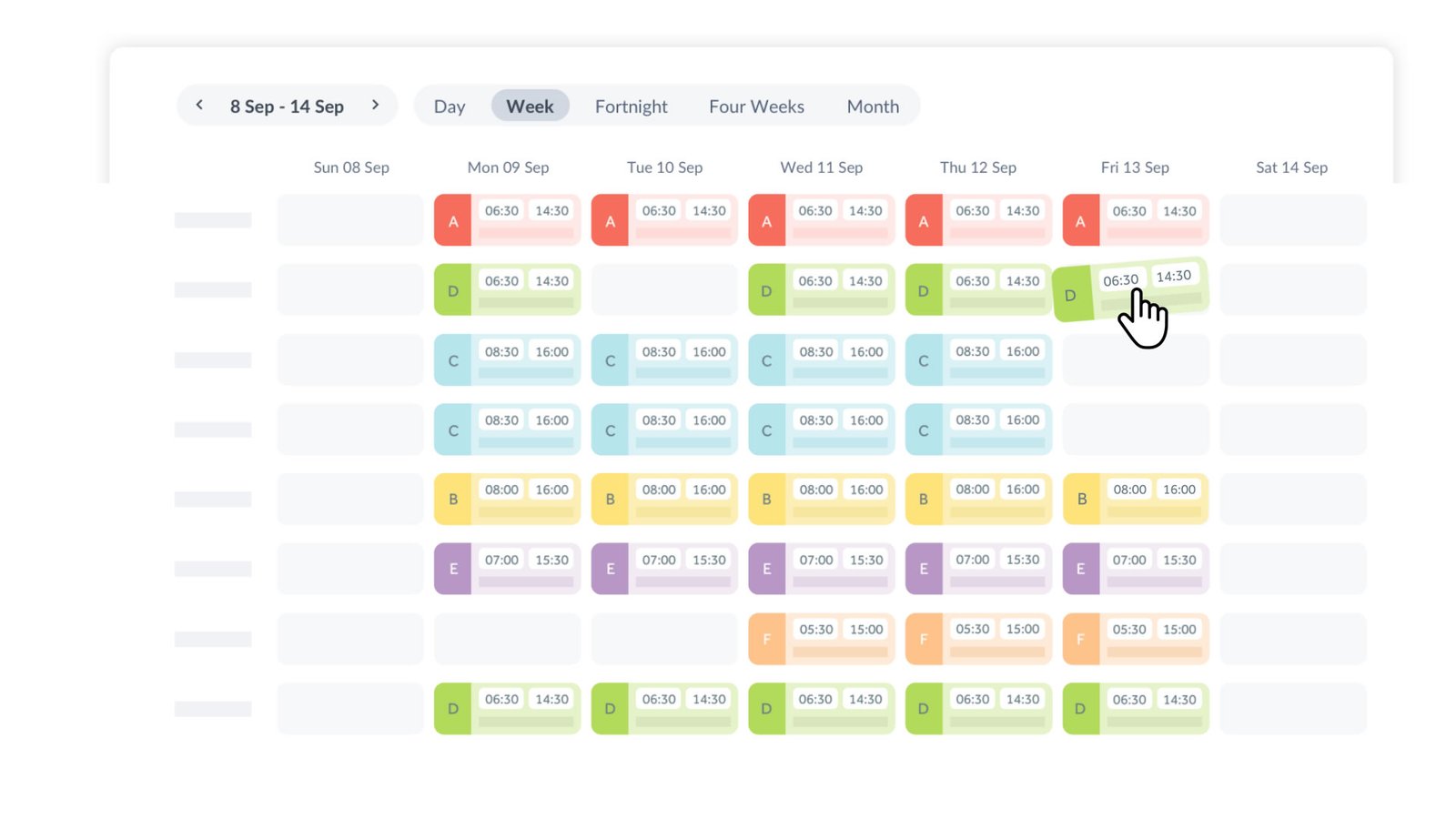
Instead of rotas taking 4 hours per week to create, it now only takes 15 minutes for managers to build a schedule for their staff. “I’m a bit of a rota queen,” says Jaine who has 34 years experience in the care industry. Initially, there was concern about how to share rotas with the staff but says she’s never had a problem and that her team couldn’t live without Workforce.
Increased visibility for managers
“We’re using Workforce as a tool to manage an ever-growing level of staff and being able to see everything that’s going on in the business is much clearer now that what we had” said James Finance Manager at Glenholme. With Workforce.com, Glenholme Care Group has much more visibility of their workforce including when staff clock in and out, staff leave requests & leave balances, and even enables team members to update employee details on their own, allowing managers to focus their time where it is needed.
Improving staff satisfaction
Initially, managers at Glenholme were unsure if staff would use Workforce.com but after introducing the user-friendly app, even the most technologically hesitant staff navigate it effortlessly, saving valuable time, reducing frustration and eliminating the need for extensive training. Consequently, this newfound efficiency significantly bolstered staff morale, as they felt empowered and more in control of their work.
Whether a home manages 20 staff or 2000, Workforce.com helps optimise staff performance and operations, ensuring exceptional quality of care is provided.

Content provided by Workforce.com. For more information please visit www.workforce.com.
Managing chronic pain in Greenwich - Kairos Rehabilitation - Dr David McGavin & Dr Ellen Wright
 Introduction
Introduction
There are few effective treatments for chronic pain. Medication often adds little and may even harm (viz the opioid crisis) and resources for non-pharmaceutical approaches are limited. Furthermore, chronic pain cannot be targeted as a single illness, like diabetes, because it is so often complicated by other long-term conditions, social issues and polypharmacy.
Kairos Rehabilitation Trust is a small anthroposophic1 medical charity, funded by the NHS, which has been working in Greenwich for 12 years. 120-140 patients with chronic pain are treated each year, referred by their GPs via the local MSK hub. The emphasis is on working with the patient in a rehabilitation program, rather than just against the condition, which has not previously responded to usual treatments.
The team consists of a GPwSI in chronic pain and 3 anthroposophically trained therapists.
- The GP receives, explains, coordinates therapies and reviews progress regularly.
- Rhythmical Massage is a gentle, restorative and enlivening method which often induces sleep, proving that sleep is possible.
- Eurythmy Therapy is a harmonious form of movement, where one learns to move more confidently again and without pain. It can be practiced at home.
- Anthroposophic1 art therapy is guided experimentation with colour and form. It broadens awareness of oneself and the world and builds self-esteem.
All anthroposophic1 therapies take account of where the person is in the healing process, needing care and protection at first and thereafter gradual, increasing and appropriate challenge. Therapy sessions last an hour, are all 1:1, and weekly for 6 weeks. A GP review follows, with referral to the next therapy or to an exit interview if appropriate. Social group activities include a weekly choir, art group and patient-led discussion group.
 Evaluation and Cost
Evaluation and Cost
Evaluation shows significant reduction in patient-reported pain severity, depression and improvement in quality of life.2 There was also a reduction in medication and specialist appointments and improved social integration. Costs average about £1500 per patient for one year of treatment including all GP and therapy appointments.
We see many patients that have been referred to us ‘as a last resort’. In this situation we have noticed 3 common factors liable to obstruct progress:
1 Exhaustion: Ongoing tiredness undermines clear thinking and decision making, mood and motivation. All chronic pain and mental health conditions are exaggerated by exhaustion. Finding sleep and energy are therefore high priorities. The bodily therapies described above can induce relaxation and increase vitality.
An initial simple warm ginger compress applied to the spine is often quickly helpful in reducing pain. Its effect may last for up to a few days and it can be taught to continue at home. Massage commonly induces sleep, revealing that it can be possible. Several home tips and remedies promote sleep adding to the impetus of the therapies.
A change of symptoms or just feeling ‘more together’ after therapy always surprises. It encourages and engenders enthusiasm, adding new hope of attaining improvement.
2 Unhelpful habits: Habits make life possible but valuable habits drilled in when well can get in the way when one becomes chronically ill. It is naive, especially with someone exhausted or living in chaos, to expect more than short term change with cognitive methods alone.
Rhythmical massage moves fluid inclusively throughout the body. A tense stiff lower back may thereby be gradually persuaded to belong again within general spinal function. Eurythmy teaches how to bring movement and balance more consciously through the affected area. Little by little, the musculature can be encouraged to soften and re-integrate.
Even small improvements raise hope and enthusiasm that replace old responses (like requests for different medication) with new ones, (like new interests and seeking supportive company).
3 Wariness of doctors: This is particularly relevant when dealing with patients who have become defensive. Over recent years GPs have become distanced from patients. It is harder to consistently see the same doctor, one who knows one well enough to take one’s particular circumstances into account. Mutual trust can no longer be taken for granted. Furthermore, GPs’ aims for safety, economy and getting the job done quickly don’t necessarily coincide with the patient’s hopes and needs.
If the patient has found confidence to take the lead, co-managing their path and/or reducing medication, things are straight forward. But for those who are daunted, frightened of change or who have become protective of their condition, preparatory work will be needed to avoid resistance, stalemate and even acrimony.
1Gunver S. Kienle et al. Anthroposophic medicine: An integrative medical system originating in Europe. Global Adv Health Med 2013;2(6):12.
2Wright et al A clinical evaluation of a community-based rehabilitation and social intervention programme for patients with chronic pain and associated multi-morbidity. J Pain Manage 2017;10(2):00-00.
Content provided by Dr David McGavin – GpwSI in Chronic Pain Management and Medical Director of Kairos
Dr Ellen Wright – GP and Clinical Academic Fellow, Trustee of Kairos
For more information please email This email address is being protected from spambots. You need JavaScript enabled to view it.
Healthcare Integration in the NHS: Fall Prevention and Gait Rehabilitation - Dynamic Metris Ltd
The NHS aims to be at the forefront of integrating innovative healthcare solutions to enhance patient care and streamline services. The GaitSmart rehabilitation exercise programme is one such innovative solution, helping older adults reduce their risk of falls or recover from joint replacement. Walking is a fundamental aspect of healthy living and one of the few medical fields where technology is rarely used. GaitSmart provides a unique solution to help people walk better.
GaitSmart is revolutionising the way falls prevention and joint replacement rehabilitation is delivered, offering a groundbreaking digital solution that enhances mobility and quality of life. With 20% of the global population affected by MSK issues, which are a leading cause of falls in the elderly and significant workday losses, the need for innovative treatment methods is critical.
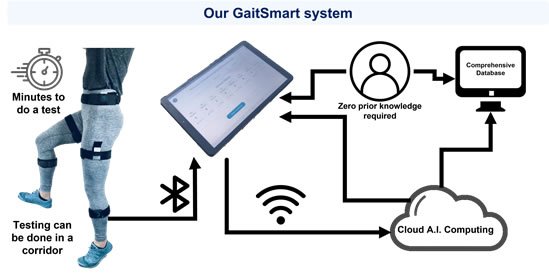
GaitSmart is a sensor-based clinical tool that provides an accurate assessment of a patient’s gait kinematics. Using a visual traffic light system and scoring, it presents easy-to-understand data for both clinicians and patients. This system not only identifies the severity and location of gait issues but also offers a personalised exercise rehabilitation program based on objective data. A healthcare assistant can administer the test in just 10 minutes, making it a highly efficient solution. Our four-session strength and balance program over 12 weeks has been shown to improve mobility and quality of life for patients with various MSK conditions.
All the evidence was independently reviewed and in recognition of its efficacy and economic viability, GaitSmart was awarded NICE Guidance in 2024 for Falls Prevention. GaitSmart is a Class 1m medical device, fully certified to be used in the UK, Europe, US and Canada.
How does GaitSmart work?
The quick and easy-to-use GaitSmart test can be administered by non-professional healthcare workers with minimal training, freeing up scarce physiotherapy resources. GaitSmart’s digital test results allow easy retrieval of patient information and the ability to track changes in mobility over time.
Step 1: Wireless Inertial Measurement Unit (IMU) sensors are attached to the individual.
Step 2: The individual walks 10strides while the sensors record the motion.
Step 3: The GaitSmart Report shows key gait kinematic parameters and overall GaitSmart Scores.
 The GaitSmart Report and Personalised Exercise Plan
The GaitSmart Report and Personalised Exercise Plan
The GaitSmart report shows the ranges of motion that the patient can achieve at their hip and knee joints, the amount of out-of-plane movement through adduction and abduction, as well as the symmetry of the lower limbs. Gait issues are highlighted in the GaitSmart Report with the severity being denoted by simple traffic light colour-coding. The GaitSmart Report also provides a personalised exercise programme to address the muscle weaknesses identified. This total solution empowers the individual and motivates them to perform their exercises at home.
GaitSmart in Clinical Practice
Traditional physiotherapy solutions, while effective, are often costly and resource-intensive and lack objective data to tailor treatments accurately. Unlike conventional methods and virtual physiotherapy apps, GaitSmart delivers precise, objective assessments and personalised exercise plans, filling a crucial gap in the market. This technology addresses the inherent challenges of monitoring gait and offers a complete solution that supports patient health and wellbeing.
GaitSmart represents a valuable treatment option that could also address a significant gap in gait rehabilitation services. Traditional rehabilitation often requires substantial time and skilled resources, which can limit accessibility for some patients. GaitSmart, delivered by trained healthcare assistants, offers a more accessible and less resource-intensive alternative. This is particularly beneficial for patients who may not otherwise have access to dedicated gait rehabilitation services due to logistical or financial constraints. Training healthcare assistants to deliver GaitSmart ensures that patients receive consistent and effective rehabilitation while maintaining a streamlined and cost-effective service delivery model. This is particularly beneficial in community settings where access to physiotherapists may be limited. The integration of GaitSmart within the NHS thus exemplifies a collaborative approach to healthcare delivery, optimizing the use of available resources and enhancing patient care.
In the UK alone, over 20 million people suffer from MSK conditions, including 8 million with osteoarthritis. Each year, more than 200,000 undergo joint replacements, and over 3 million people over 65 experience falls primarily due to poor gait. GaitSmart provides an invaluable tool for these individuals, offering a digital solution that surpasses the limitations of existing physiotherapy and digital health options.
Implementing GaitSmart
NICE Guidance [MTG78] states GaitSmart can be utilized to help adults at risk of falls, with gait and mobility issues. This is crucial as falls are a significant concern, with around 10.8 million people over 65 at risk of falls, of which around 3.3 million fall each year. Falls can lead to severe health complications, including fractures and reduced quality of life. GaitSmart offers a proactive approach to mitigating these risks by improving gait stability and mobility.
Recovering a normal gait after injury or surgery is crucial for maintaining mobility and overall health. Traditional gait monitoring, typically conducted in specialized gait laboratories, is often costly and time-consuming, limiting its accessibility to many patients and typically only those in the post-operative phase. This restricted access can result in suboptimal recovery for those undergoing knee and hip replacements, impacting their long-term health. GaitSmart offers a cost-effective and efficient solution that can be delivered both in clinics and the community. By providing accessible gait monitoring and intervention, GaitSmart supports not only post-operative recovery but also prevention and pre-operation care. This comprehensive approach ensures that individuals on waiting lists, as well as those undergoing preventive measures, receive the necessary support to maintain and improve their gait. Aligning with the NHS Long Term Prevention Programme, GaitSmart enhances patient outcomes across all stages of care, promoting better long-term health and mobility.
GaitSmart in the NHS
GaitSmart is supported by a decade of clinical trials. The published clinical evidence supporting GaitSmart has been collected from a range of NHS settings across primary, secondary, and community care. The evidence shows that GaitSmart can improve gait parameters and patient-reported outcomes for people over a very wide age range, including those with limited mobility and using a range of walking aids. It also provides greater independence to individuals whilst also reducing the burden on the NHS. As GaitSmart is a medical device with a digital component, it supports the NHS’s commitment to evidence-based practice. It also provides objective data that can be shared across primary, secondary, and community care, in a similar way to a simple blood pressure reading. This supports the ‘Integrated Care’ strategy and ensures a continuum of care for all patients.
By providing a proactive, data-driven approach to gait rehabilitation, GaitSmart not only improves patient outcomes but also represents a cost-effective solution for the NHS. Its integration into healthcare services marks a significant step forward in addressing the challenges of MSK conditions and enhancing patient care.
Content provided by Dynamic Metrics Ltd. For more information please visit www.dynamicmetrics.com.