



The CompreHensive geriAtRician-lead MEdication Review (CHARMER) hospital deprescribing intervention: What it means for primary care - Sion Scott, Lecturer in Behavioural Medicine & Debi Bhattacharya, Professor of Behavioural Medicine, University of Leices
Background
The National Overprescribing Review (NOR) estimates that 10% of medicines prescribed are inappropriate either because they are unnecessary or harmful(1). Deprescribing is the process of a healthcare professional working in partnership with the patient and/or caregiver to identify and discontinue inappropriate medicines(2). Deprescribing may either be ‘reactive’, in response to medication-related harm that has already happened, or ‘proactive’, in order to prevent medication-related harm from happening as illustrated by Figure 1.
Inappropriate medicines are associated with a range of adverse outcomes including morbidity, hospitalisation and mortality(3). Systematic reviews of randomised controlled trials demonstrate that proactive deprescribing is safe and associated with positive patient and health system outcomes(4–6). Accordingly, there is a need to embed proactive deprescribing into routine practice to prevent harm and unnecessary health resource use.
The NOR advocates a system-wide approach to tackling overprescribing; primary care setting has responded with significant policy and practice change(1). For example, the introduction of structured medication reviews in 2020 which require primary care organisations to target patients who are at high risk of being prescribed unnecessary or harmful medicines(7).
An admission to hospital is another opportunity to identify and deprescribe inappropriate medicines, complementing the strategies in primary care(8). An estimated 1 in 2 people aged ≥65 years admitted to hospital are prescribed at least one medicine that should be deprescribed(9). However, research undertaken by the CHARMER team demonstrates that virtually no proactive deprescribing occurs during a hospital admission(10). This is despite over 9 in 10 older hospital patients and caregivers stating that they would be willing to have a medicine deprescribed during a hospital admission(11).
There are a number of compelling reasons to bring the hospital setting into the fold to support tackling overprescribing including the presence of geriatricians and pharmacists who are experts in older people and medicines respectively, and the facility to intensively monitor a patient’s response to deprescribing(8). However, as with all healthcare settings, there are a number of barriers and enablers to proactive deprescribing in hospital that require addressing before it becomes routine practice.

Figure 1: A comparison of reactive and proactive deprescribing
The CHARMER intervention
CHARMER is a deprescribing intervention aimed at increasing proactive deprescribing undertaken by geriatricians and pharmacists in hospitals in England. Five years of funding was awarded by the National Institute for Health and Care Research (NIHR) to develop the CHARMER intervention and test its effectiveness and cost-effectiveness. The CHARMER intervention does not direct clinical decision-making; it is designed to address the practical and social factors that geriatricians and pharmacists say hinder proactive deprescribing in hospital. For example, one barrier is that geriatricians and pharmacists feel that patients may be resistant to having a medicine deprescribed in hospital, despite evidence to the contrary(11). CHARMER therefore includes a component designed to address this barrier; video case studies demonstrating geriatricians successfully navigating deprescribing consultations with patients and caregivers. Figure 2 provides a summary of the five components of the CHARMER intervention.

Figure 2: Five components of the CHARMER intervention
The CHARMER feasibility study was completed in 2022 and concluded that implementing the intervention in NHS hospitals and conducting a definitive trial was feasible(12). 1st February 2024 marked the commencement of the CHARMER definitive trial. The trial involves 24 acute hospitals listed in Figure 3, over 100 geriatricians and pharmacists and 24,000 patients admitted to Older People’s Medicine wards. The primary outcome measure for the trial is a reduction in 90-day hospital readmission.
What CHARMER means for primary care
Whilst CHARMER is a hospital-based intervention, any change in hospital deprescribing activity will impact on other settings within the healthcare system, principally primary care. Early in the CHARMER programme, a Primary Care Advisory Group (PCAG) was established including membership from the following:
- Medical directors and clinical pharmacists of Integrated Care Systems
- Directors and Prescribing Leads of Integrated Care Systems (ICSs)
- Directors of Primary Care Networks (PCNs)
- Commissioners of Primary Care Medicine Services
- Senior GPs and pharmacists with a role or interest in medicines optimisation
The PCAG provides strategic oversight by identifying and advising on any potential barriers and enablers in primary care relevant for successfully implementing CHARMER and maximising return to the healthcare system. Communication at the transfer of care, maintenance and monitoring of deprescribing post-discharge have been extensively considered by the PCAG and CHARMER team.
If the CHARMER intervention is effective, primary care teams will see patients being discharged from hospital with more medicines deprescribed than historical rates. Some deprescribing will not require any further action from primary care teams, however clear communication including a rationale for deprescribing in the discharge communication is essential to prevent uncertainty and potential re-prescribing owing to a gap in information. There may be instances where deprescribing has happened in hospital which requires a degree of minoring by primary care, or where gradual deprescribing has been initiated in hospital which requires primary care to take over. This is similar to situations where medicines are started in hospital that require follow-up by primary care. In both instances, in addition to the aforementioned communication, hospital teams must ensure that the information provided in the discharge communication is comprehensive and supports primary care colleagues to maintain hospital-initiated deprescribing.
There is significant variation in transfer of care between hospitals and primary care across the country and this is likely to be reflected in the CHARMER trial. This presents both a risk and an opportunity to CHARMER. Poor transfer of care increases the chances of failing to realise the gains from successful deprescribing in hospital. Transfer of care that facilitates maintenance of deprescribing and ongoing monitoring where necessary is imperative to realising any benefits from CHARMER in addressing national overprescribing.
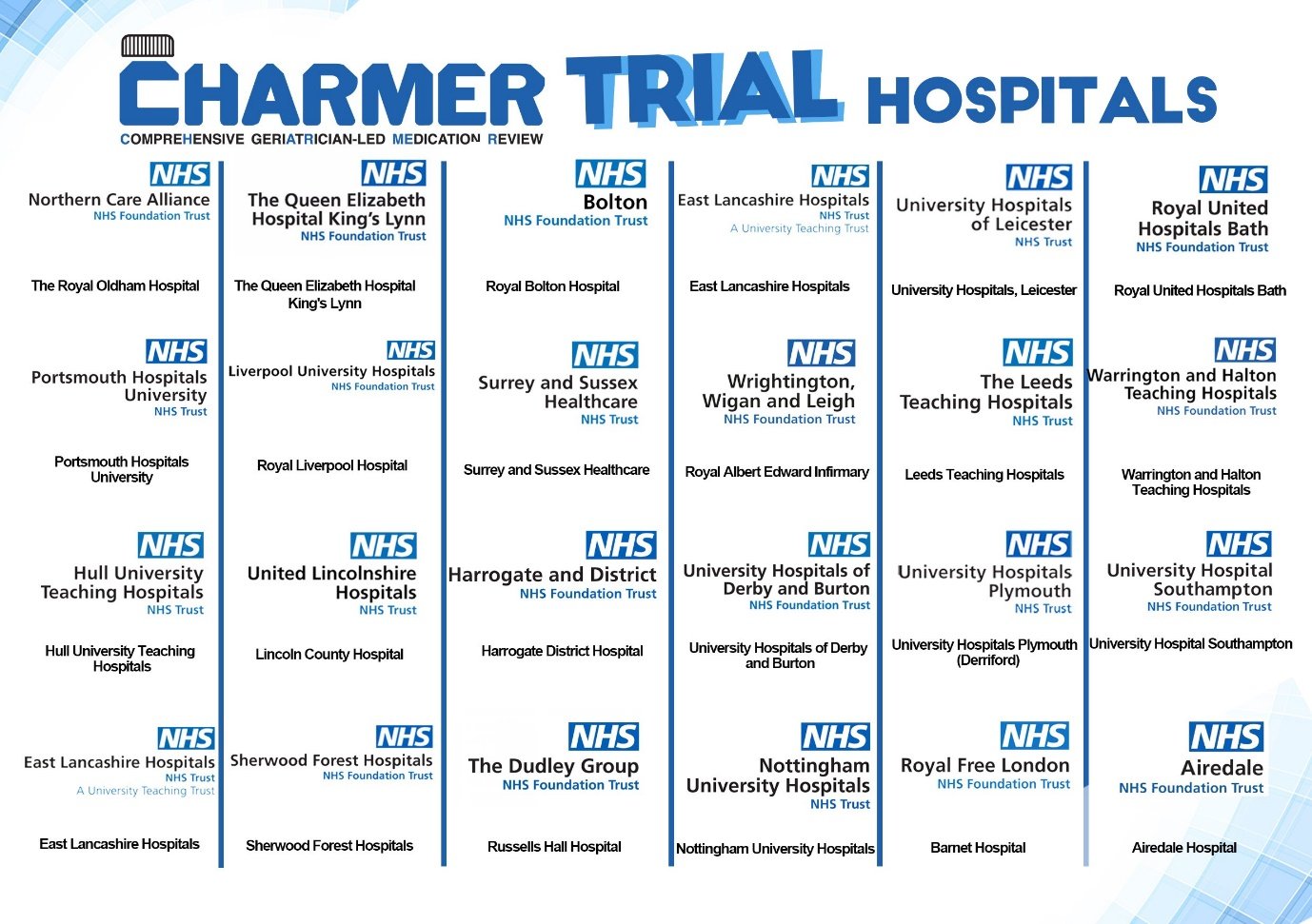
Figure 3: The 24 hospitals participating in the CHARMER trial
Primary care investing in maintaining hospital initiated deprescribing can help foster a system-wide approach to tackling overprescribing in the NHS and maximise the benefits of CHARMER. All primary care colleagues for whom a patient is discharged from a CHARMER hospital and has been enrolled in the trial will be invited to provide feedback on the impact of the intervention. Discharge communication will be annotated to inform primary care of the patient’s enrolment in the trial and will include an invitation to provide feedback The CHARMER team are interested in all feedback its impact, either positive or negative. In the event that you are likely to receive patients who are discharged from the care of one of the CHARMER hospitals, please look out for the invitation in the discharge communication.
For more information about the CHARMER programme of research, visit www.charmerstudy.org, email This email address is being protected from spambots. You need JavaScript enabled to view it. and follow us on X: @CHARMER_Study.
References
- Good for you, good for us, good for everybody: A plan to reduce overprescribing to make patient care better and safer, support the NHS, and reduce carbon emissions [Internet]. Department of Health and Social Care; 2021 [cited 2021 Dec 21]. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1019475/good-for-you-good-for-us-good-for-everybody.pdf
- Woodward MC. Deprescribing: achieving better health outcomes for older people through reducing medications. J Pharm Pract Res. 2003;33(4):323–8.
- Spinewine A, Schmader KE, Barber N, Hughes C, Lapane KL, Swine C, et al. Appropriate prescribing in elderly people: how well can it be measured and optimised? The Lancet. 2007;370(9582):173–84.
- Bloomfield HE, Greer N, Linsky AM, Bolduc J, Naidl T, Vardeny O, et al. Deprescribing for community-dwelling older adults: a systematic review and meta-analysis. J Gen Intern Med. 2020;35(11):3323–32.
- Page AT, Clifford RM, Potter K, Schwartz D, Etherton-Beer CD. The feasibility and effect of deprescribing in older adults on mortality and health: a systematic review and meta-analysis. Br J Clin Pharmacol. 2016;82(3):583–623.
- Thillainadesan J, Gnjidic D, Green S, Hilmer SN. Impact of deprescribing interventions in older hospitalised patients on prescribing and clinical outcomes: a systematic review of randomised trials. Drugs Aging. 2018;35(4):303–19.
- Network Contract Directed Enhanced Service Structured medication reviews and medicines optimisation: guidance [Internet]. [cited 2022 Oct 6]. Available from: https://www.england.nhs.uk/wp-content/uploads/2021/03/B0431-network-contract-des-smr-and-mo-guidance-21-22.pdf
- Scott S, Twigg MJ, Clark A, Farrow C, May H, Patel M, et al. Development of a hospital deprescribing implementation framework: a focus group study with geriatricians and pharmacists. Age Ageing. 2020;49(1):102–10.
- Gallagher P, Lang PO, Cherubini A, Topinková E, Cruz-Jentoft A, Montero Errasquín B, et al. Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitals. Eur J Clin Pharmacol. 2011;67(11):1175–88.
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Deprescribing admission medication at a UK teaching hospital; a report on quantity and nature of activity. Int J Clin Pharm. 2018;40(5):991–6.
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Attitudinal predictors of older peoples’ and caregivers’ desire to deprescribe in hospital. BMC Geriatr. 2019;19(1):1–11.
- Scott S, Atkins B, Martin-Kerry JM, Pritchard M, Alldred DP, Clark AB, et al. CompreHensive geriAtRician-led MEdication Review (CHARMER): protocol for a feasibility study of a hospital deprescribing behaviour change intervention. BMJ Open. 2023 Aug 1;13(8):e075795.
Content provided by Sion Scott, Lecturer in Behavioural Medicine, University of Leicester & Debi Bhattacharya, Professor of Behavioural Medicine, University of Leicester
For more information visit www.charmerstudy.org, or email This email address is being protected from spambots. You need JavaScript enabled to view it..



