



Applying behavioural science to shape quality improvement - Debi Bhattacharya, Professor of Behavioural Medicine, University of Leicester & Sion Scott, Lecturer in Behavioural Medicine, University of Leicester
An ever-growing body of research evidence means that our clinical practice is required to constantly evolve in response to emerging evidence. The result feels like yet a new ‘ask’ every financial year layered on top of our already stretched workforce. However, it is our professional responsibility to ensure that healthcare innovations that demonstrate cost-effectiveness in the trial setting are translated into practice.
Implementation of a novel healthcare innovation into routine practice requires us to change established patterns of behaviour(1). Problems can arise if the innovation is counter to established patterns of behavioural, professional or personal norms. This can lead to disparity between best practice according to the evidence and the care received by our patients.
Despite significant efforts by practitioners and organisations, suboptimal translation of healthcare innovations into practice is a long standing and well-established problem, resulting in a ‘translational gap’ between the evidence base and realities of practice(2). A 2003 Lancet article revealed that up to 40% of the care delivered to patients in developed countries is not according to present scientific evidence and that 20% to 25% of patients receive unnecessary or harmful care(3).
Strategies to promote implementation of new healthcare innovations have traditionally focussed on providing information and training to practitioners. Whilst these address gaps in knowledge and skills, changing behaviour is a complex process determined by several influencing and interacting factors, all of which require consideration. The NHS long-term plan and national overprescribing review are recent examples of national policy highlighting the need for changes to practice(4).
Shared decision-making
The NHS long-term plan committed to making personalised care routine practice and in March 2022, launched the Primary Care Network, Directed Enhanced Service called: Personalised Care: Social prescribing; shared decision making; digitising personalised care and support planning. Personalised care comprises the following six components:
- Shared decision making
- Personalised care and support planning
- Enabling choice, including legal rights to choice
- Social prescribing and community-based support
- Supported self-management
- Personal health budgets and integrated personal budgets.
The first component of routinising Shared Decision Making (SDM) requires the most extensive behaviour change as it affects all practitioners involved in health care related consultations. Figure 1 illustrates the expected role of the practitioner in facilitating the patient to be an active partner in the decision making about all of their health and care related decisions. There is wide recognition that achieving this is ambitious. In our previous article we outlined how, simply asking people what needs to happen to lead them to change their behaviour does not capture the full picture because people will tend to focus on the need for more resource and training . Other potentially powerful barriers and enablers can play an important role in determining whether a person changes their behaviour.

Figure 1: The principles of shared decision making
Numerous behaviour change theories are available to structure how we develop an implementation strategy to support the required change in behaviour of people. The Theoretical Domains Framework(5) draws together many behaviour-change theories and outlines fourteen factors that can influence behaviour such as a person’s beliefs about the repercussions of attempting to or not attempting to incorporate SDM in their consultations, what they think that colleagues and patients think about the idea of SDM, and how confident they feel about incorporating SDM in their consultations. The Personalised Medicine Directed Enhanced Service is accompanied by a framework to support SDM implementation which is reproduced in Figure 2.
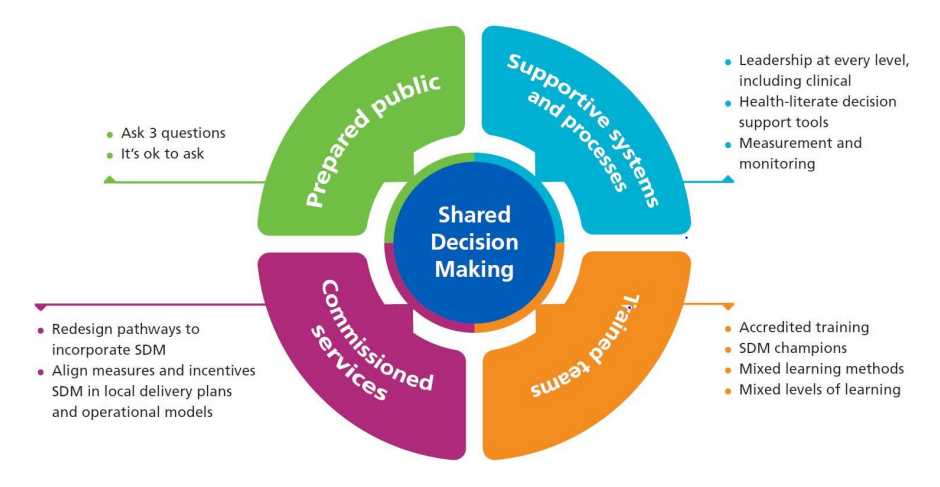
Figure 2 NHS England shared decision-making Implementation Framework (reproduced from ‘Personalised Care: Shared Decision-Making Summary guide(6))
The four listed components may address all fourteen factors that can influence behaviour. What is needed, is for each ICS to establish the finer detail of the barriers and enablers of their practitioners implementing SDM. This will allow ICSs to tailor each of the four components of the implementation framework to their own needs as they can be designed to change behaviour through a variety of mechanisms.
Prepared public
This includes messaging to the public to empower them to ask questions and participate in decision making when it is offered. Examples of how a prepared public can facilitate practitioners to engage in SDM include, by asking questions they can act as a prompt or a positive social influence by making the practitioner feel that SDM is an expectation. By being receptive to practitioner attempts of SDM, they may motivate the practitioner to persist in attempting SDM.
Supportive systems and processes
This includes access to decision support tools which could make SDM more convenient for the practitioner by making the required tools more accessible and thereby reducing cognitive burden and time commitment. If embedded into prescribing systems, the could even be configured to act as prompts to the prescriber to facilitate SDM.
It also includes leadership, however, guidance regarding the most salient messaging from leadership to elicit behaviour change is necessary. For example, if a large proportion of ICS practitioners feel that their patient population will not be responsive to SDM, then the messaging at leadership level will need to focus on that element.
Trained teams
Whilst training at its most superficial level is designed to give people the required skills to undertake a behaviour It can also be used as a vehicle for addressing numerous other barriers and enablers to behaviour change such as increasing confidence, addressing misconceptions and generating motivation to deliver an expected role.
Commissioned services
When the barriers and enablers associated with teams’ capability and capacity to undertake a new behaviour such as facilitating SDM have been addressed, incentives and benchmarking practice can change behaviour through making SDM a goal that practitioners are motivated to achieve. Perhaps the most recognisable application of incentivisation to change behaviour in primary care is the Quality and Outcomes Framework, which sets goals for example to reduce prescribing of a certain medicine by an a priori set proportion.
Where to go from here?
A survey to help ICSs identify the key barriers and enablers to implementing SDM within their organisation is available on the NIHR East of England Applied Research website.
References
- Davis DA, Taylor-Vaisey A. Translating guidelines into practice: a systematic review of theoretic concepts, practical experience and research evidence in the adoption of clinical practice guidelines. Cmaj. 1997;157(4):408–16.
- Haines A, Donald A. Making better use of research findings. Bmj. 1998;317(7150):72–5.
- Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. The lancet. 2003;362(9391):1225–30.
- Baker R, Camosso-Stefinovic J, Gillies C, Shaw EJ, Cheater F, Flottorp S, et al. Tailored interventions to address determinants of practice. Cochrane Database of Systematic Reviews. 2015;(4).
- Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science. 2017;12(1):1–18.
- Personalised Care, Shared Decision Making, Summary guide, Shared Decision Making team within the Personalised Care Group. Shared Decision Making Summary guide. NHS England and NHS Improvement;
Content provided by Debi Bhattacharya, Professor of Behavioural Medicine, University of Leicester & Sion Scott, Lecturer in Behavioural Medicine, University of Leicester



