



A spotlight on Pulse Oximetry - Not all pulse oximeters are created equally! - Dr. Basil Matta MA FRCA FFICM, Senior Medical Director, Masimo
 The first commercially available pulse oximeter, a life-saving device that clipped on a finger and showed the level of oxygen in blood, was invented by Dr. Takuo Aoyagi, a Japanese Bioengineer in 1974. Monitoring of blood oxygen saturation is one of the greatest advances in patient monitoring and the introduction of this technology coincided with a 90% reduction in anesthesia-related fatalities. Over the course of the past almost 50 years, the ability to detect oxygen saturation levels has become as important if not more important that the other 4 vital signs—temperature, blood pressure, pulse rate, and respiratory rate.
The first commercially available pulse oximeter, a life-saving device that clipped on a finger and showed the level of oxygen in blood, was invented by Dr. Takuo Aoyagi, a Japanese Bioengineer in 1974. Monitoring of blood oxygen saturation is one of the greatest advances in patient monitoring and the introduction of this technology coincided with a 90% reduction in anesthesia-related fatalities. Over the course of the past almost 50 years, the ability to detect oxygen saturation levels has become as important if not more important that the other 4 vital signs—temperature, blood pressure, pulse rate, and respiratory rate.
COVID-19 has shone a spotlight on this most important measurement in medical practice, with media outlets suddenly showing interest in these devices. The demand, influenced by COVID-19, has also led to many less efficacious pulse oximeters being marketed and bought by lay people as well as poorly informed health care providers. The vast majority of these poor quality oximeters have not undergone proper testing and their performance falls far short of what is expected from hospital grade devices that are designed to prevent serious deterioration and death.
With heightened awareness of pulse oximetry technology, more scrutiny has been applied to the devices in the market. Some of the discoveries have concluded that even some of the currently available hospital grade oximeters perform poorly under certain conditions, particularly common in small children and sick patients. Many “conventional” pulse oximeters work under the assumption that only arterial blood is pulsatile. This is a sound assumption when the person/patient is not moving and has good perfusion, but fails to give an accurate reading when you need it most – when the patient is moving such as the case in small children and/or when the patient has poor perfusion due to cold hands or because the patient is very ill. Under these conditions, a conventional pulse oximeter is likely to display false (low or high) SpO2 readings and inaccurate pulse rates resulting in high incidence of false alarms. These false/inaccurate readings can also lead to clinical interventions that are not appropriate.
Masimo Signal Extraction Technology (SET®) has been designed to overcome the limitations of conventional pulse oximetry. Masimo SET® technology is trusted by care providers around the world – it is used to monitor more than 200 million patients each year, and has been shown in more than 100 independent and objective studies to outperform other pulse oximetry technologies, providing clinicians with unmatched sensitivity and specificity to make critical patient care decisions. This same tried and tested high quality technology (Masimo SET® pulse oximetry) is now available in the home for spot check and continuous measurement of oxygen saturations.
In addition to motion and low perfusion (cold hands or poor circulation), racial bias, where oxygen saturation readings are lower in dark skin patients, has been highlighted as an important issue and a possible factor in the increased mortality rate seen in ethnic patients who contracted COVID-19. This was a surprise to us at Masimo, as we have been calibrating our pulse oximeters using desaturation testing in both dark and light skinned subjects for over two decades. This recent focus on racial bias prompted us to re-examine our internal data and evaluate prospectively the accuracy, precision, and bias of the Masimo MightySat® with Masimo SET® pulse oximetry. In our analysis we used a rigorous study protocol and data interpretation paradigm. Our results indicated that the accuracy precision and bias between white and black patients monitored with Masimo MightySat® with Masimo SET® pulse oximetry was similar for all SaO2 readings and samples obtained during sequential desaturation in the range 100-70% oxygen saturation. Therefore, the recent retrospective reports of occult hypoxemia having racial bias do not apply to the Masimo MightySat® with Masimo SET® pulse oximetry. Patients, families and healthcare providers can rest assured that SpO2 values obtained from Masimo MightySat® with Masimo SET® pulse oximetry are accurate and free of racial bias. For more information please see www.masimo.co.uk/company/news/pulse-oximetry-racial-bias.

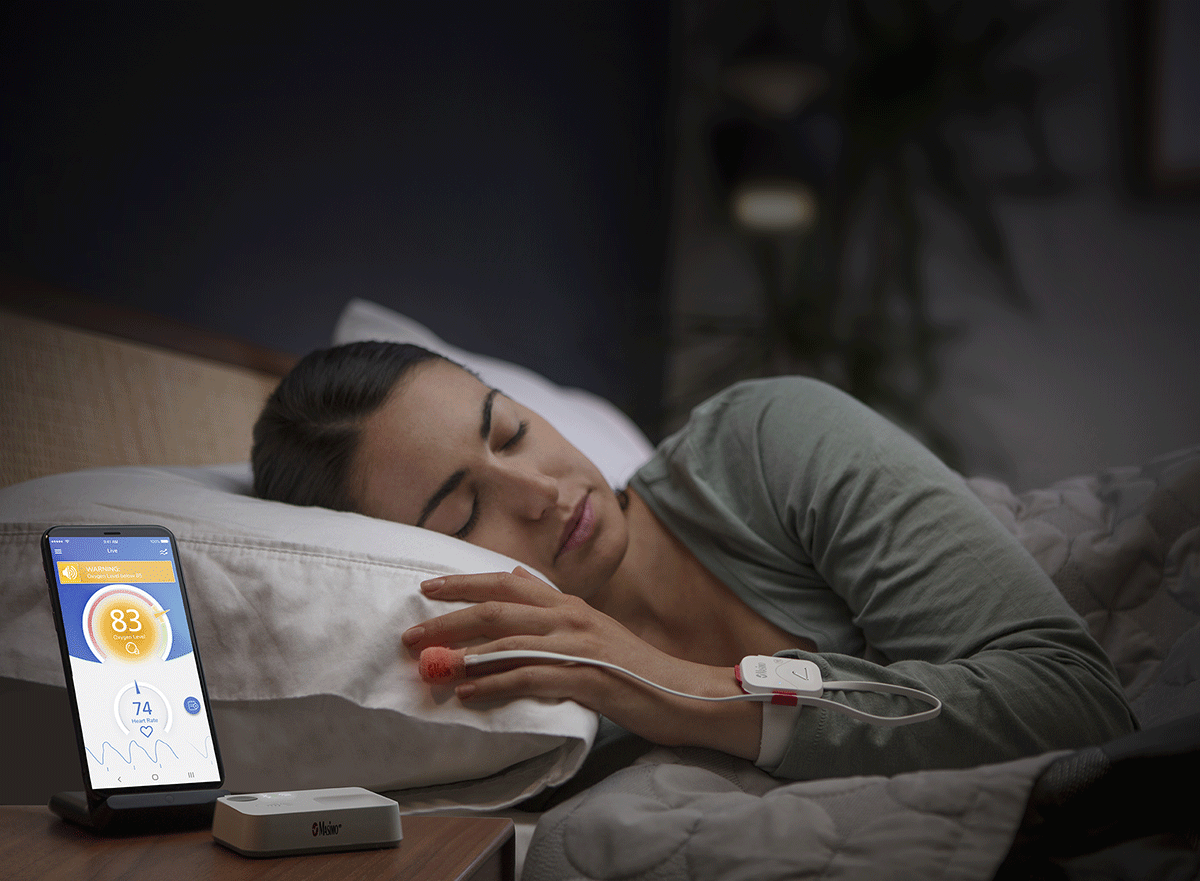
There is now evidence to suggest that continuous pulse oximetry monitoring is beneficial in detecting episodes of desaturation when patients are asleep – even at home, with hospital grade technology. Our Masimo SafetyNet® with Masimo SET® pulse oximetry is a remote monitoring solution that now provides the clinician with the ability to monitor patients while they are at home – thereby reducing hospital admissions without degrading care. The Masimo SafetyNet® Alert version of this remote monitoring solution allows “self-monitoring” by the individual, with alerts to wake the individual should oxygen saturations drop. Further sustained drops in saturations lead to text alerts being sent to a next of kin or designated health provider, and even a call to emergency services.


Dr. Basil Matta, Senior Medical Director for Masimo, is the immediate past Divisional Director for Musculoskeletal, Digestive Diseases, Major Trauma and Perioperative Care Medicine at Cambridge University Hospitals NHS, where he is a Consultant in Anaesthesia & Critical Care, and Affiliate Assistant Professor at the University of Cambridge.
Email: This email address is being protected from spambots. You need JavaScript enabled to view it.



